
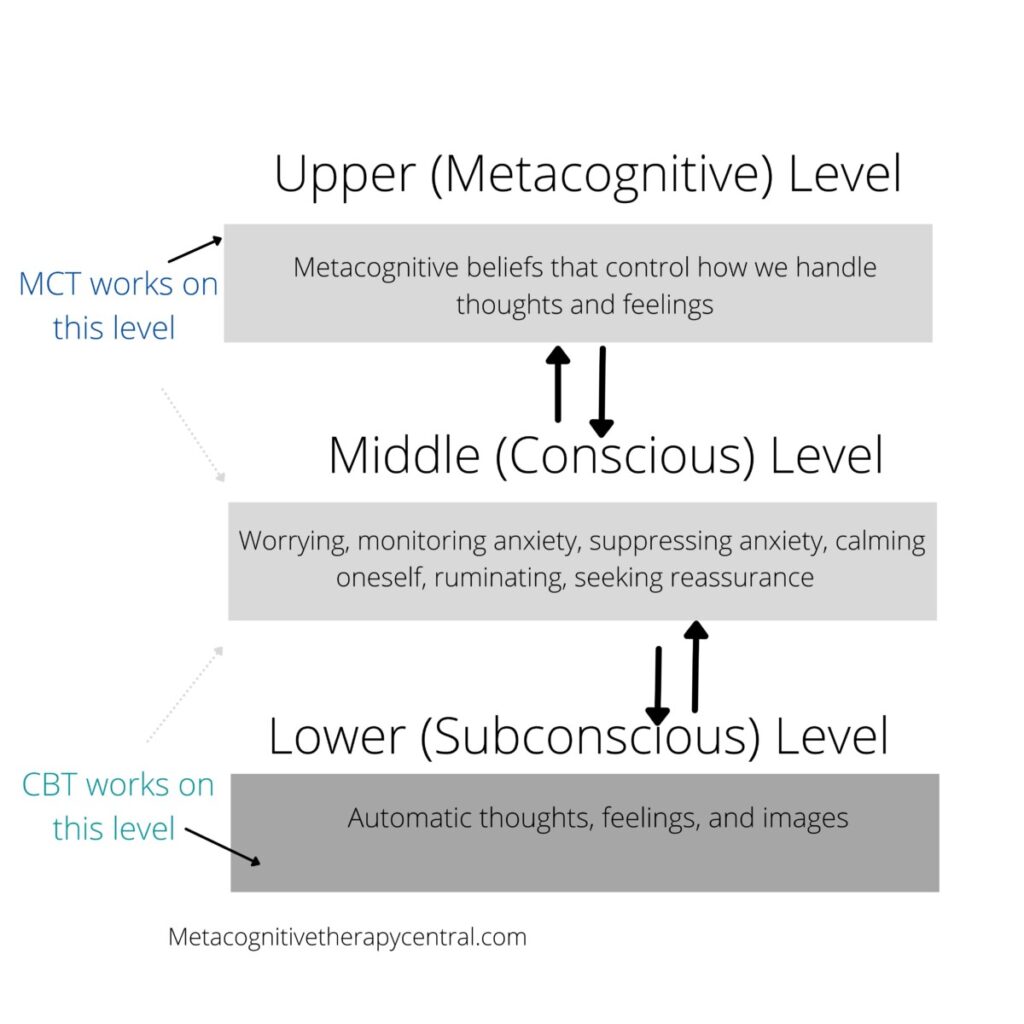
Metacognitive therapy (MCT) and Cognitive-behavioral therapy (CBT) have very different views of the mechanisms that cause mental illness. This is also reflected in each treatment’s level of effectiveness.
Results from a recent meta-analysis show that MCT creates a greater reduction in worry and decreased anxiety symptoms in patients with generalized anxiety disorder, compared to CBT. Similar results are seen for depression, where MCT is found to be more effective than CBT.
Both treatments target the mechanisms they believe cause and maintain mental illness. According to CBT that mechanism is the content of negative thoughts and self-beliefs, whereas in MCT, it is the CAS (consisting of rumination and worry, biased attention, and other thought control strategies) and metacognitive beliefs (beliefs about the way our thinking works).
The question is whether MCT has a more accurate understanding of what causes mental illness and this may be the reason why it is more effective than CBT. But how exactly does this difference affect the treatment of people with anxiety and depression?
| CBT (Cognitive-behavioral therapy) | MCT (Metacognitive therapy) | |
| Cause of mental illness | The content of negative thoughts and self-beliefs (schemas) | The CAS and the metacognitive beliefs responsible for activating CAS (CAS = rumination, worry, threat-monitoring, etc.) |
| The role of thoughts in mental illness | Thoughts by themselves lead to mental illness (for example, anxiety, depression, OCD) | Thoughts are brief passing events in the mind and not facts |
| Treatment focus | Challenge the content of negative thoughts and self-beliefs and replace them with more realistic thoughts Change unhelpful behavior | Reduce CAS and challenge the beliefs people have about their thinking (metacognitive beliefs) |
MCT helps patients relate to unwanted thoughts as passing events in the mind and separate from reality. CBT challenges the content of unwanted thoughts and beliefs about oneself and the world.
What makes MCT an effective treatment?
- MCT changes how we relate to thoughts and feelings. Rather than fusing them with reality and testing their validity, we can learn to put less importance on thoughts.
- MCT teaches us that we can learn to control our attention and move it around the way we want. That helps us let go of unhelpful overthinking patterns and choose what version of reality we want to inhabit.
- MCT changes false metacognitive beliefs about thoughts and feelings so that we believe more in our ability to stop worry and rumination.
- Changed metacognitive beliefs prevent future setbacks.
- MCT teaches new ways to relate to thoughts that are done through both understanding (declarative knowledge) and through exercises (procedural knowledge). That way, these new techniques are easier to remember when in need.
How is MCT different from CBT?
MCT is different from CBT because it doesn’t work with the content of thoughts but aims to change false metacognitive beliefs and reduce overthinking. CBT focuses on changing the thoughts we experience from negative to more realistic ones, as well as pointing out cognitive distortions like, for example, black-and-white thinking, that are thought to bias thinking and fuel anxiety or depression.
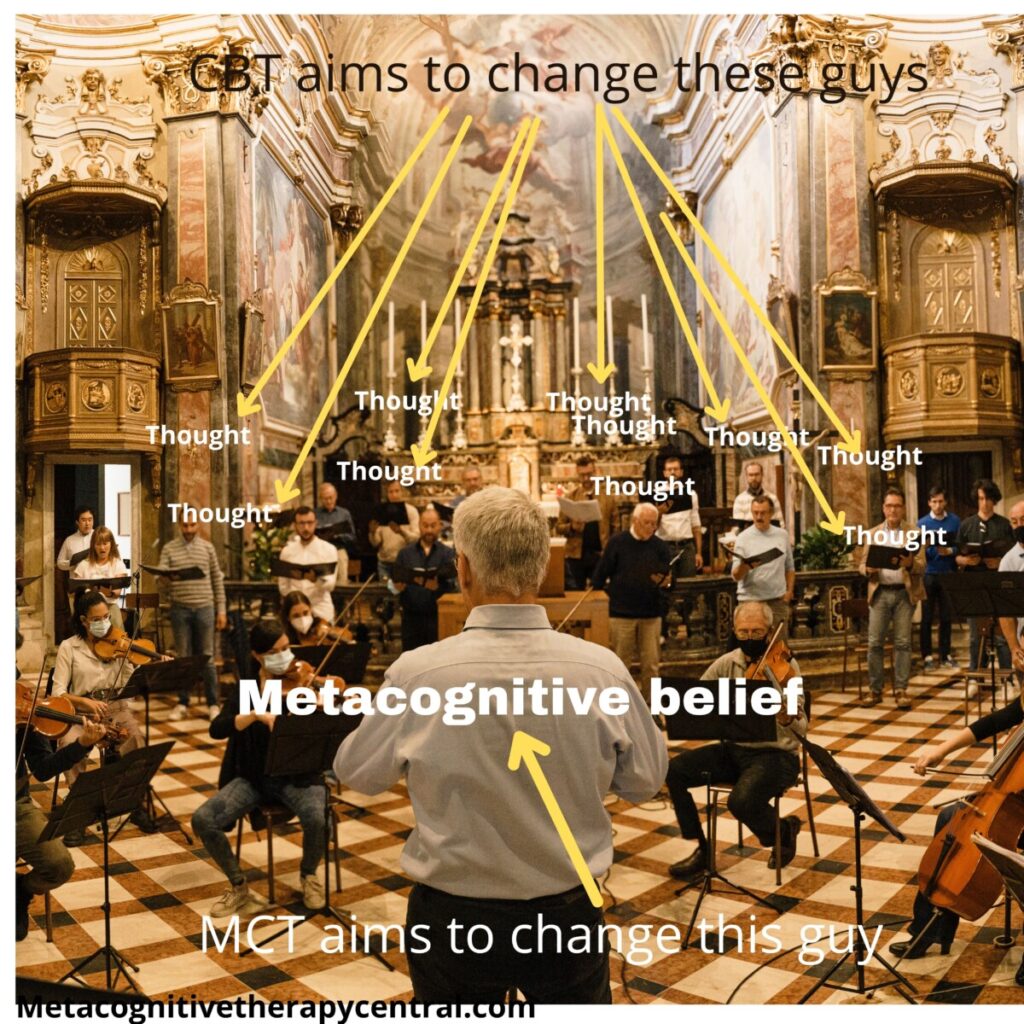
Imagine that the mind is a large orchestra playing its instruments. CBT treatment’s goal equals stopping specific instruments from playing. In comparison, MCT won’t get involved in which instruments are playing. Instead, MCT challenges the role of the conductor that monitors and controls the production of a good overture.
How MCT explains mental illness
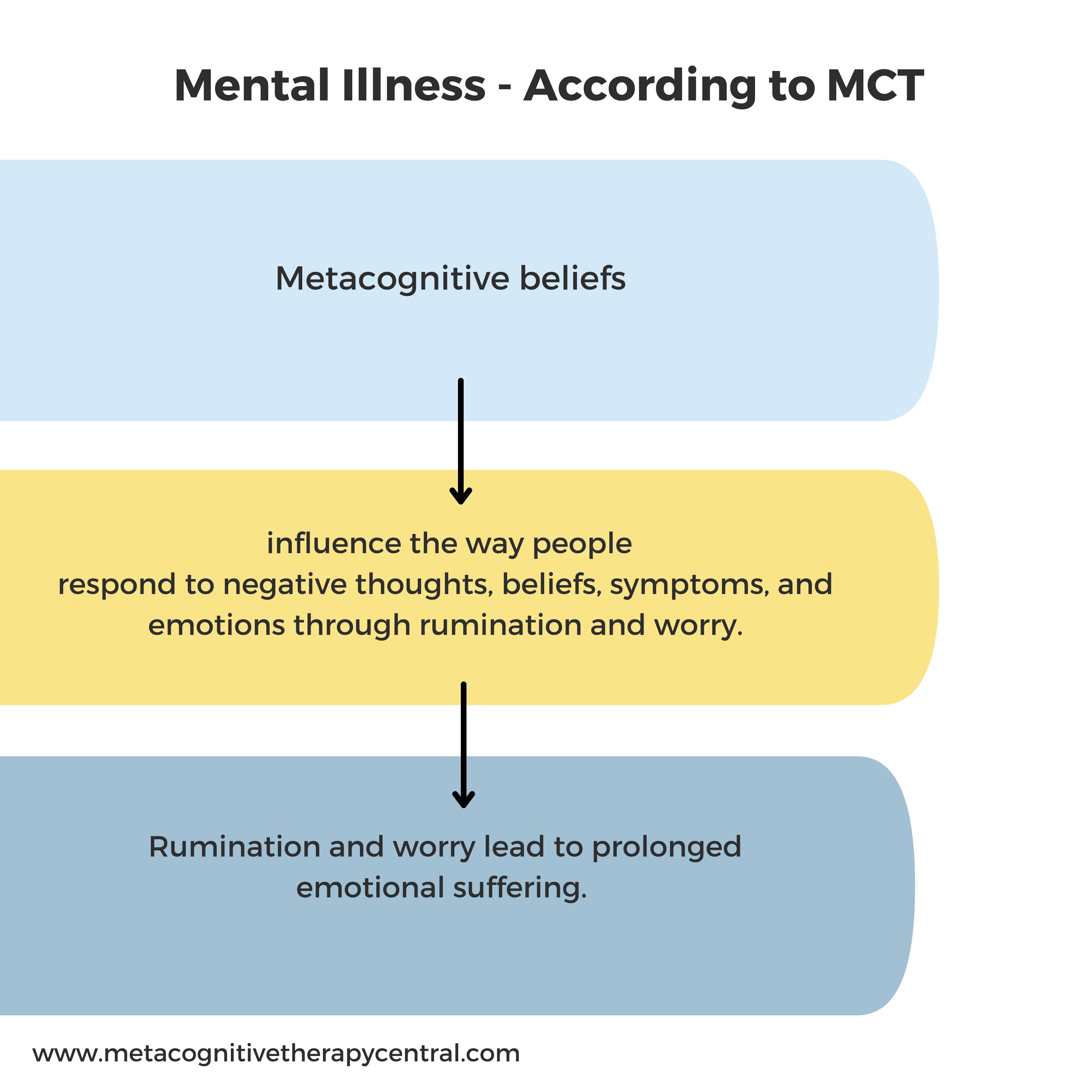
According to Metacognitive therapy, anxiety, depression, and other mental disorders are caused by overthinking. Overthinking, in the form of repetitive thinking styles like rumination and worry, prolongs negative thoughts and feelings and affects emotional states such as anxiety or depression. Rumination and worry are controlled by metacognitive beliefs (beliefs about thinking).
Examples of metacognitive beliefs are:
I need to analyze my thoughts to understand why I feel this way
Worrying helps me be prepared
I can’t control worry/rumination
Worrying is harmful
The goal of MCT treatment is to reduce the time spent on rumination and worry and alter the metacognitive beliefs that activate them. An important part of MCT is that worry and rumination can be controlled (contrary to CBT, where worry and rumination are seen as automatic and reflexive symptoms of mental illness).
How metacognitive beliefs activate worry and rumination
Let’s go back to the orchestra description.
After playing for days, the musicians in the orchestra are tired, groggy, and unable to concentrate. Maybe they need to rest more before their next performance. But the conductor (metacognitive beliefs) continues to instruct the musicians to play (worrying and ruminating). As a result, the musicians get stressed, sad, and demotivated (worrying and ruminating lead to low mood, anxiety, and depression).
MCT tries to recognize the behavior of the orchestra and change it to a more helpful one:
How much time does the orchestra play (time spent ruminating and worrying)? Can the time be reduced to half an hour instead of endless hours of performance? (prolonged worrying and ruminating extends negative emotions and tires the brain’s other functions like working memory and problem-solving ability).
MCT also challenges the conductors’ need to make the musicians constantly play (how useful is worrying and ruminating?). And more importantly, does the conductor believe that he can control his musicians? (can ruminating and worrying be stopped?).
Once the conductor realizes that there are more advantages to letting the musicians rest (they will be less tired and moody), AND he believes that the musicians are able to follow his instructions, he sets the orchestra up for success (recovery from anxiety and depression).
What are thoughts in MCT?
Metacognitive therapy works on the metacognitive level, also called the metacognitive mode. In the metacognitive mode, thoughts are viewed as brief passing events separate from reality. This means that having unwanted or intrusive thoughts are not facts or directly reflect the person experiencing them.
For example, a person who suffers from OCD is able to experience his thoughts in two different ways:
- Thoughts experienced in object mode When seeing a stain in a public place, Tim has the thought: “It’s contaminated with feces“. Tim does not differentiate between the thought and the stain. To him, the problem is the stain, not that he has a thought about the stain.
- Thoughts experienced in metacognitive mode When Tim sees the stain, he is aware that he also has a thought in his mind about the stain, and he can separate the two. Thoughts are passing events in his mind and he doesn’t need to respond to them. Therefore, in the metacognitive mode, the problem is not the stain but how much Tim chooses to engage with the thought about the stain.
When thoughts are experienced in object mode, they are given too much importance, which becomes problematic when people worry or ruminate about them for too long. This can then lead to an increased frequency of negative thoughts, failed efforts to get rid of them, and emotional distress.
MCT works in the metacognitive mode and teaches people that thoughts are brief events in the mind that we don’t need to respond to. An MCT therapist will therefore ask his patient: “How much time do you spend analyzing the thought that the floor is contaminated? How does that help you? Can you reduce that activity?”
Content of thoughts in MCT
The content of thoughts in MCT is unimportant and separate from reality. Instead, the amount of time people spend ruminating about these thoughts is more important and needs to be reduced.
The MCT therapist views the patient’s problem (depression, for example) as caused by extended overthinking, inflexible attention, and counterproductive control strategies like thought suppression. These thinking strategies are part of the cognitive attentional syndrome, CAS. In MCT, the content of thoughts is not important for achieving recovery, regardless of what it is.
Whether the patient has thoughts like “I am stupid and worthless” or “I am getting fired” doesn’t matter. What matters is that the patient ruminates and worries about their thoughts and that rumination and worry need to be stopped to recover from depression.
Since metacognitive beliefs control worry and rumination, the MCT therapist’s goal is also to change the patient’s metacognitive beliefs.
Examples of metacognitive beliefs in depression are:
Ruminating about why I feel down will help me find solutions
I can’t control ruminations
Depression is a chemical imbalance in my brain
Therefore, the goal of the MCT therapist is to identify and challenge the patient’s metacognitive beliefs:
“You believe that rumination will help you find answers to your depression. Is that really the case, or have you become even more depressed when ruminating?“
“If you can’t control rumination, how does it ever stop when someone interrupts you?“
Attention in MCT
According to MCT, attention plays a central role in mental illness. When people ruminate and worry, they focus their attention inward instead of focusing on their surroundings. This self-focused attention reinforces worry and rumination and makes people with mental illness monitor for threats. In MCT, this is called inflexible attention.
Examples of self-focused attention:
- For example, people with panic disorder constantly pay attention to signs of anxiety to prevent future panic episodes.
- People with illness anxiety monitor their bodies for signs of serious illness.
- People with social anxiety turn their attention inward when entering a feared social situation. They use self-focused attention to prevent making an unfavorable impression on others by monitoring their behaviors and worrying.
Self-focused attention blocks healthy emotion processing and hinders disconfirmation of false metacognitive beliefs (that anxiety is harmless and that social anxiety is not a hindrance to socializing).
However, focusing attention on “threats” limits people’s access to information that corrects false ideas in feared situations.
MCT teaches patients to use attention flexibly and has developed two techniques that help achieve flexible attention; Attention Training Technique (ATT) and Situational Attentional Refocusing (SAR).
ATT is external focusing on different sounds through selective attention, attention switching, and divided attention. ATT is practiced at specific set times and is not used as a coping technique when experiencing discomfort.
Attention Training Technique is associated with improvements in symptoms in panic disorder, illness anxiety, and depression. Neurologically, it can reduce activity in the amygdala (the part of the brain responsible for processing threatening and fearful information).
SAR is used to redirect attention when exposed to anxiety-provoking situations. That way, patients gain new information from the external environment to correct false beliefs. For example, people with panic disorder learn that reducing threat-monitoring (monitoring for signs of panic) and redirecting attention to neutral information helps them notice their anxiety less.
Attention modification is used in MCT to remove unhelpful coping strategies (like worry, rumination, and threat monitoring) and challenge false metacognitive beliefs.
Attention is the basis of consciousness and of learning about the self and the world (Adrian Wells, founder of Metacognitive therapy)

How CBT explains mental illness
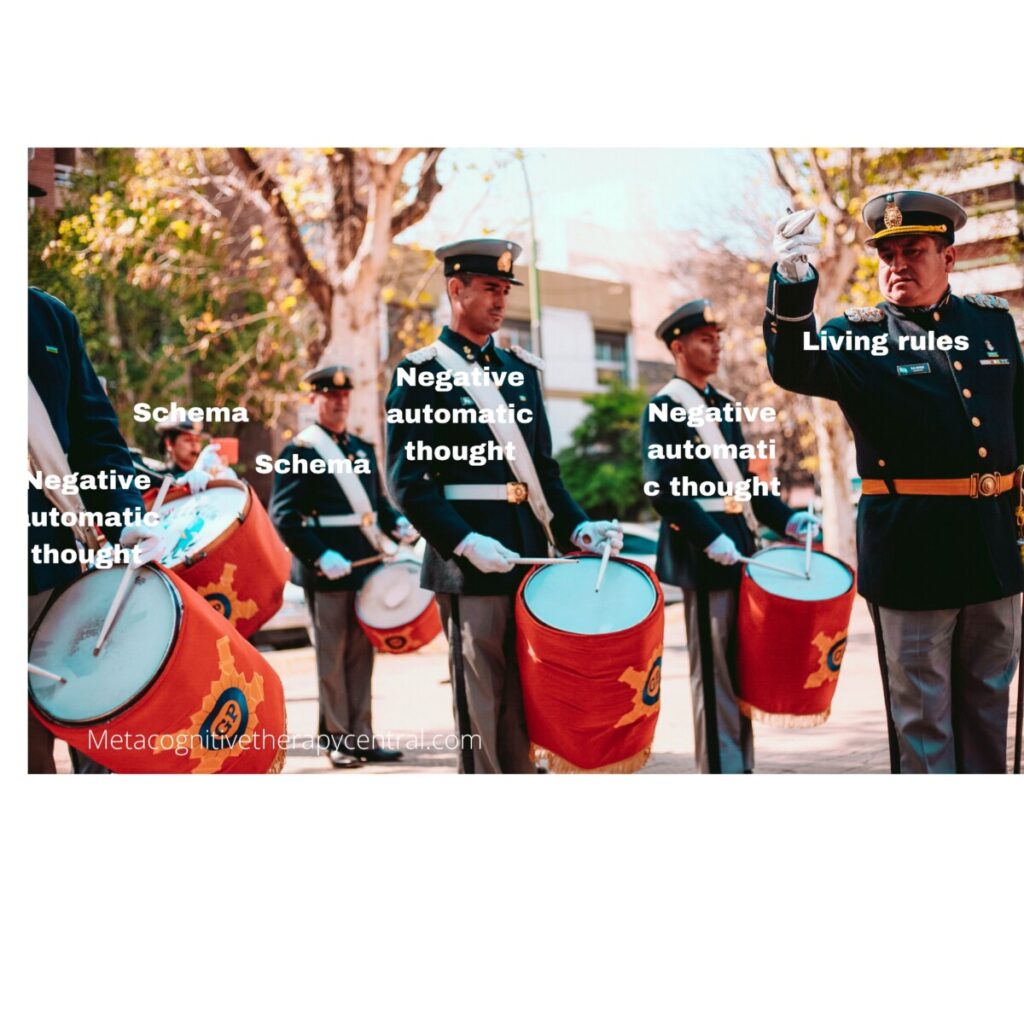
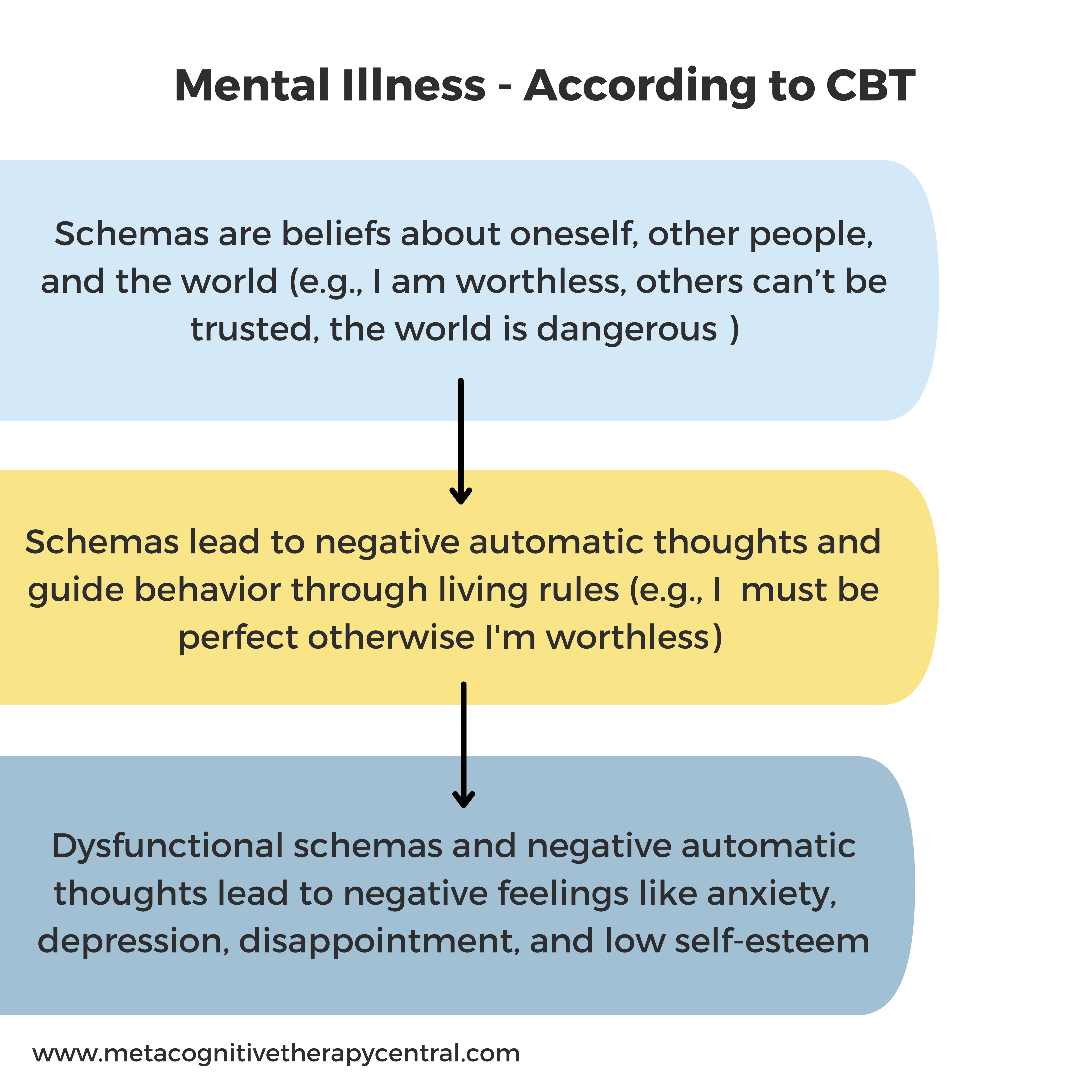
In CBT, thoughts can impact emotions and behavior. Cognition (thinking) is divided into negative automatic thoughts and schemas (beliefs about oneself and the world). According to CBT, schemas are general underlying beliefs that give rise to negative automatic thoughts and are the reason behind psychological disorders because they generate negative emotions and affect behavior.
The schemas also affect the production of negative automatic thoughts like “Something is wrong” or “Are they thinking something bad about me?“.
For example, someone with a schema, “I am worthless” may experience negative automatic thoughts like “I will probably be rejected” in a situation where they are about to ask someone on a date. According to CBT, this negative automatic thought will cause feelings of sadness and lead to inactivity and depression.
CBT also identifies certain dysfunctional assumptions that some people live by. Dysfunctional assumptions are rigid, conditional ‘rules for living’ that people adopt, for example, “I have to be perfect, or else I am a failure” is a rule some people live by. Another example of a living rule is “I have to be liked by everyone, or I am worthless.”
According to CBT, living rules exist because of people’s schemas. It is however not clear, how schemas lead to negative automatic thoughts or how negative automatic thoughts cause mental illnesses like anxiety and depression.
CBT treatment focuses on identifying negative automatic thoughts, challenging their validity, and replacing them with more accurate ones.
In the orchestra metaphor, according to CBT, there is no conductor. And if there is one, he is on the same level as all the other musicians, but he has been there the longest. No one else controls the musicians (there are no metacognitive beliefs in CBT).
What are thoughts in CBT?
In CBT, thoughts are experienced as indistinguishable from real-life events. For example, a person can have the thought “I am worthless” and experience it as a piece of direct data. Because of this, he is more likely to respond to the thought by analyzing it: “Why am I this way? What can I do to change?”
A thought like “I am a failure” might be inaccurate, but in CBT, a person with that thought acts as if it were true. This is because thoughts in CBT are experienced as valid and a reflection of reality. CBT views the thoughts at the object level.
A CBT therapist places a lot of importance on thoughts through questioning and analyzing the patient’s thoughts in therapy. The therapist questions the validity of her patient’s thoughts by asking: “What is the evidence that you are worthless?” In CBT, there is no direct separation between the person and the thought.
Content of thoughts in CBT
The content of thoughts in CBT (what thoughts say and mean) is important and closely related to reality.
A CBT therapist is interested in the content of the patient’s thoughts. If the patient has the thought, “I am useless“, the therapist helps the patient to reality test the content of this thought.
The CBT therapist is also interested in identifying thinking errors in the patient’s thinking. Examples of thinking errors are black-and-white thinking (either I am good or bad), discounting the positive (I only passed the exam due to luck), and emotional reasoning (my thought must be true because I feel bad).
Schemas (“I am worthless” and “The world is a dangerous place“) are challenged and changed the same way negative automatic thoughts are. Therefore, CBT doesn’t differentiate between schemas and negative automatic thoughts in regard to the way they are challenged. To CBT, they are all thoughts, and their content matters a great deal.
Attention in CBT
When attentional strategies are used in CBT, the goal is to distract the patient from unwanted thoughts, feelings, and pain. Attention in CBT is used as a coping technique.
Attention training is often mentioned in the “New wave” generation of cognitive-behavioral therapies. For example, Acceptance and Commitment Therapy (ACT) teaches self-focused attention. The goal here is to expose patients to distressing feelings to reduce the strength of the feeling (desensitization).
In Mindfulness-Based Cognitive Therapy (MBCT), attention training is used as a part of meditation to redirect focus on the breath whenever patients are distracted by unwanted thoughts.
This type of attention training is different from the attention training technique (ATT) in MCT.
Conclusion – The difference between CBT and MCT
According to CBT, when a student fails his exam and gets the thought “I am a failure“, he becomes depressed because of that thought. According to MCT, the student becomes depressed because he ruminates about this thought.
Basically, the view of the mind in MCT is different than the one in CBT. MCT distinguishes between thoughts and metacognitive beliefs, whereas CBT does not recognize metacognitive beliefs but divides thoughts into different categories (negative automatic thoughts, dysfunctional assumptions, and schemas). Schemas are not part of a higher-level belief system (like metacognitive beliefs are in MCT). Instead, schemas are the content of thoughts, just like negative automatic thoughts.
MCT, therefore, focuses on changing metacognitive beliefs so that people stop worrying and ruminating. CBT analyzes and changes the content of thoughts.
CBT uses attention to help escape or minimize distressing thoughts, feelings, and pain. MCT uses the Attention Training Technique to counteract self-focus, reduce worry and rumination, and change false metacognitive beliefs. MCT also uses attention to correct misinformation about threats.
CBT cannot answer why two failing students can have the same thought, but only one gets depressed.
Is MCT better than CBT?
Both CBT and MCT are effective treatments, but research shows that MCT shows 18% better effects than CBT for depression and 19% for anxiety
There is increasing evidence that Metacognitive therapy is a more effective treatment than CBT. For example, CBT for generalized anxiety disorder has produced modest outcomes, and research shows that CBT’s effect is declining. Only 38% recover from anxiety with CBT compared to 57% in MCT. More than 50% don’t recover from anxiety in CBT treatment. The newest research comparing MCT with CBT for depression shows that 74% recover from depression with MCT, compared with 56% with CBT.
Why is MCT better than CBT?
The success of MCT compared to CBT is due to several factors. According to researchers, one of the weaknesses of CBT is that it uses many different treatment techniques combined but with a limited understanding of how each technique works. No one knows exactly how each CBT technique contributes to helping patients recover from mental illness. Besides, CBT doesn’t clearly define the nature of mental disorders such as anxiety and depression, which further leads to the lack of knowledge about what precisely improves it.
MCT, on the other hand, has a very specific understanding of mental illness.
MCT’s view on mental illness is based on a few tightly defined variables (overthinking, unhelpful coping strategies, and metacognitive beliefs). In MCT, all psychological disorders can be explained by this model, which is a simple model and makes it easy to measure its effect as well as treat a variety of mental disorders (anxiety, depression, social phobia, and OCD) through a few techniques.
Since worry and rumination cause most mental disorders and MCT can reduce worry and rumination effectively, MCT can be universally applied across all mental disorders. There is no need to come up with new techniques for different mental disorders, making MCT time-consuming and cost-effective.
Why is CBT less effective than MCT?
There are many types of Cognitive-behavioral therapies. Some of these CBTs have specific and evidence-based models of psychological disorder, while others don’t.
Since CBT believes that schemas are the root of psychological disorders, each disorder has a variety of underlying schemas. According to Wells, one of the limits of CBT is that you can come up with a new schema to fit any disorder. There are two reasons why this is ineffective.
- Too many different schemas can be extensive to challenge in therapy. How does the therapist know which one to challenge? And in what order?
- Too many schemas broaden CBT’s definition of psychological disorder. A lack of a clear understanding of mental disorders makes them harder to treat, compromising CBT’s treatment success.
Final thoughts on MCT vs. CBT
Some researchers argue that the effect experienced from CBT treatment is due to the indirect change in metacognitive beliefs. During CBT treatment, knowing and identifying negative automatic thoughts might help some patients stop worrying and ruminating about them. This sometimes results in changes in metacognitive beliefs (that worrying can be controlled).
Since Metacognitive therapy (MCT) is a cognitive therapy, many mistakenly assume it is a new type of cognitive-behavioral therapy (CBT), a so-called “Third-wave” cognitive therapy. However, MCT is not a type of CBT. In MCT, all mental disorders are caused by higher-level metacognitive beliefs that control overthinking, whereas CBT only works on the level of thoughts. Metacognitive beliefs are not mentioned in any cognitive-behavioral therapies, making MCT a theoretically different therapy than CBT.
Are you interested in Metacognitive therapy?
You can book a free intro session and learn how MCT can specifically help you in your situation. During this session, a metacognitive case formulation and a treatment plan will be created for you and you can have all your questions answered. The offer is non-binding.
References
- Callesen P, Reeves D, Heal C, Wells A. Metacognitive Therapy versus Cognitive Behaviour Therapy in Adults with Major Depression: A Parallel Single-Blind Randomised Trial. Sci Rep. 2020 May 12;10(1):7878. doi: 10.1038/s41598-020-64577-1. Erratum in: Sci Rep. 2020 Jul 7;10(1):11460. PMID: 32398710; PMCID: PMC7217821.
- Solem S, Wells A, Kennair LEO, Hagen R, Nordahl H, Hjemdal O. Metacognitive therapy versus cognitive-behavioral therapy in adults with generalized anxiety disorder: A 9-year follow-up study. Brain Behav. 2021 Oct;11(10):e2358. doi: 10.1002/brb3.2358. Epub 2021 Sep 14. PMID: 34520637; PMCID: PMC8553304.
- Normann N and Morina N (2018) The Efficacy of Metacognitive Therapy: A Systematic Review and Meta-Analysis. Front. Psychol. 9:2211. doi: 10.3389/fpsyg.2018.02211
- Nordahl, H. & Borkovec, T. & Hagen, R. & Kennair, L.E. & Hjemdal, O. & Solem, S. & Hansen, B. & Haseth, S. & Wells, A. (2018). Metacognitive therapy versus cognitive–behavioural therapy in adults with generalised anxiety disorder. BJPsych Open. 4. 393-400. 10.1192/bjo.2018.54.
- Schweiger JI, Kahl KG, Klein JP, Sipos V and Schweiger U (2019) Innovation in Psychotherapy, Challenges, and Opportunities: An Opinion Paper. Front. Psychol. 10:495. doi: 10.3389/fpsyg.2019.00495
- Capobianco and Nordahl, A Brief History of Metacognitive Therapy: From Cognitive Science to Clinical Practice, https://doi.org/10.1016/j.cbpra.2021.11.002
- Fisher, P., & Wells, A. (2009). Metacognitive therapy: Distinctive features. Routledge/Taylor & Francis Group.
- Solem, S., Håland, Å. T., Vogel, P. A., Hansen, B., & Wells, A. (2009). Change in metacognitions predicts outcome in obsessive–compulsive disorder patients undergoing treatment with exposure and response prevention. Behaviour research and therapy, 47(4), 301-307.


