Some people have criticized Metacognitive Therapy (MCT) for being overly promoted as a new and powerful treatment that might lose its effectiveness over time. We need to examine whether these criticisms are valid and if there’s truth to other claims made about MCT.
Critics say that MCT’s long-term effects are unclear and could be harmful. They also worry it may not handle complex issues well and that detached mindfulness, a strategy used to develop a different relationship with thoughts, could lead to suppressing them.
What is MCT? MCT, a talk therapy that targets the root causes of mental illness by focusing on a thinking style called the CAS and beliefs about thinking, called metacognitive beliefs. The CAS and metacognitive beliefs are linked to mental illness like anxiety and depression.
Metacognitive therapy’s strengths and weaknesses
| Strength | Weakness |
| MCT is built on a solid theory about what makes people mentally ill | We still don’t know how this works on a neurological level |
| MCT has proven to be effective in treating anxiety and depression and performs better than CBT | There is a need for large studies that measure this effect over the long term |
| The techniques used in therapy are individually tested and proven to reduce overthinking | The techniques require proper guidance from an experienced therapist to be used correctly |
| Metacognition (thinking about thinking) plays an important role in mental illness. This is not directly addressed in other mental health treatments | We still don’t know much about how MCT works on populations with poor metacognition |
Criticism of Metacognitive therapy – professional opinions
In Denmark, psychologists have compared MCT to CBT, expressing doubts about its effectiveness. They believe it’s too early to determine if MCT works as well as CBT because its mechanisms are not fully understood (3). Let’s look at the evidence for and against this criticism.
| Criticism of MCT: | Evidence for this criticism: | Evidence against this criticism: |
| “Not everyone can be treated with MCT because everyone is different.” | Research suggests different talk therapies have similar effects. What matters most for effectiveness is the patient’s individual needs and their relationship with the therapist (4) | This criticism lacks scientific evidence. Mental illness is often seen as a mix of biology, upbringing, and stress, but how these factors lead to it is still unclear. Research suggests that the patient-therapist relationship may not offer much more effectiveness compared to CBT alone (5) |
Most treatments for mental illness are developed by putting many techniques together. But the challenge of this is that it’s difficult to measure exactly how these techniques help overcome mental illness (6).
According to the researchers, it is more effective to build mental health treatments the following way:
- Create a coherent theory of what makes people mentally ill and test this theory
- Develop techniques specifically to match this theory and test each technique to see if it treats what it’s promised to treat
- Test this new treatment in different settings and with different populations to make sure that it works and treats mental illness effectively.
MCT is, according to these researchers, a mental health treatment that lives up to several of these standards and looks promising.
| Criticism of MCT: | Evidence for this criticism: | Evidence against this criticism: |
| “The benefits of MCT decrease over time, just like CBT.” | Research suggests CBT’s effectiveness is decreasing, especially for depression (9). It’s too early to determine MCT’s long-term impact, but factors like therapist experience and mixing MCT with other approaches may contribute to its effectiveness decline | Studies indicate that most people maintain their progress and remain recovered from anxiety disorder 3 to 9 years after receiving MCT(7)(8) |
Some researchers believe CBT’s decreasing effectiveness is because therapists mix it with other techniques like mindfulness without testing if it works.
| Criticism of MCT: | Evidence for this criticism: | Evidence against this criticism: |
| “MCT only talks about thoughts. What about emotions?” | MCT focuses on how we think, giving more importance to our thoughts than our emotions. It suggests that our thinking patterns cause mental illness | In MCT, emotions matter, but the focus is on how people handle them. Whether they worry about or suppress them. MCT addresses emotions through thoughts; for example, dwelling on unwanted emotions prolongs feeling bad |

| Criticism of MCT: | Evidence for this criticism: | Evidence against this criticism: |
| “The studies proving that MCT is effective are mainly done by researchers who are interested in its success.” | The initial studies testing MCT’s theory and techniques were primarily done by its founder, Professor Adrian Wells. He continues to actively research the effects of MCT on different mental issues. | Independent researchers are now testing how well MCT works compared to other treatments. Reviews of MCT are mainly done by researchers from different countries and not by the founder (10) (11). |
Criticism of Metacognitive therapy – public opinions
I reached out to the Instagram community for any criticisms of MCT they wanted to share. Here are some common ones and my responses based on the data available on MCT and my clinical experience from working with thousands of people.
“MCT doesn’t take low levels of neurotransmitters into consideration – talk therapy can’t fix this.”
Context: MCT focuses on how excessive worry and rumination contribute to mental illness, like depression. This contrasts with the serotonin theory, which suggests low serotonin levels cause depression.
Answer: Recent debates question whether serotonin truly causes depression. A 2019 study found insufficient evidence (1), but it faced criticism for methodological flaws (2). The authors’ quality standards, how they picked what to include, and how they explained the results all seem to have some problems. Because of this, it’s hard to trust the conclusions drawn from the study.
Regardless, these debates may overlook other factors contributing to depression, such as rumination and biased beliefs about thinking. Future research should explore how these factors interact with serotonin levels. Meanwhile, plenty of evidence supports MCT’s effectiveness in reducing rumination and overcoming depression.
Rumination is when you keep thinking about your feelings or problems. Rumination rarely leads to solutions you will act on.
“Could moving attention outward when feeling very anxious/panic have the function of avoiding unwanted sensations?”
Context: The true intention behind redirecting attention outward in MCT isn’t about avoiding emotions but rather allowing them to be felt and naturally regulate. For example, if you’re feeling panic at the gym, shifting focus back to your workout enables you to let the panic be without reacting to it.
Answer: With proper guidance from a qualified therapist, this approach can be effectively addressed and misunderstandings of how to use this strategy avoided.
“MCT does not work for people who suffer from obsessions only (intrusive thoughts/feelings/urges without performing explicit rituals)”
Context: When people have OCD, they often believe that thinking certain thoughts can make bad things happen or cause them to act on those thoughts: “Thinking this makes it so” or “Thinking this will make me act on it”. This belief leads them to take their obsessive thoughts very seriously, which leads to a lot of worrying and thinking about these thoughts. Having these beliefs about intrusive thoughts can make it harder to leave them alone.
Answer: In treating OCD with MCT, the goal is to realize that intrusive thoughts aren’t as important as they may seem. MCT helps by teaching two main things: First, thoughts aren’t always true or significant, and second, you can choose not to dwell on them.
However, some therapists, especially those new to MCT, might only focus on leaving intrusive thoughts alone without fully addressing the belief that these thoughts are important. This makes it harder to let go of obsessive thoughts if you still believe they matter. But this can easily be corrected and MCT is indeed very effective for treating OCD.

“The patient may not always know what to do after reducing worry/rumination”
Context: Some therapists help people in identifying their core values, which can serve as a compass for leading a fulfilling life, especially during tough times when dealing with difficult thoughts and emotions. Moving towards these values can bring meaning and resilience in the face of challenges. MCT does not work on identifying values but is designed to address anxiety and depressive disorders through reducing rumination and worry
Answer: I have been asked this question by some clients and in my experience, this is just another worry they are entertaining. The client is usually the expert when it comes to their life. When overthinking no longer stands in their way, they are perfectly capable of making decisions and moving towards their core values. So if this is something that you worry about, try not to engage with it and just move on with your day.
“Without knowing your values, there is no clear orientation of why you should leave negative thoughts alone”
Context: You don’t need to be guided by your values to let go of unwanted thoughts rather than worrying about them. For example, if you’re struggling with anxiety, recognizing that worrying is what exacerbates your anxious feelings should naturally prompt you to minimize worrying. Additionally, there is no clear scientific evidence suggesting that understanding your values directly leads to overcoming mental illness.
Answer: From what I have seen in my practice, and according to research, many people with mental illness want to stop worrying or ruminating, but they don’t believe they can. However, once we challenge this belief in therapy, they’re more open to leaving those thoughts alone.

“Explaining MCT to others isn’t easy because most people believe that it’s the same as distracting yourself from thoughts”
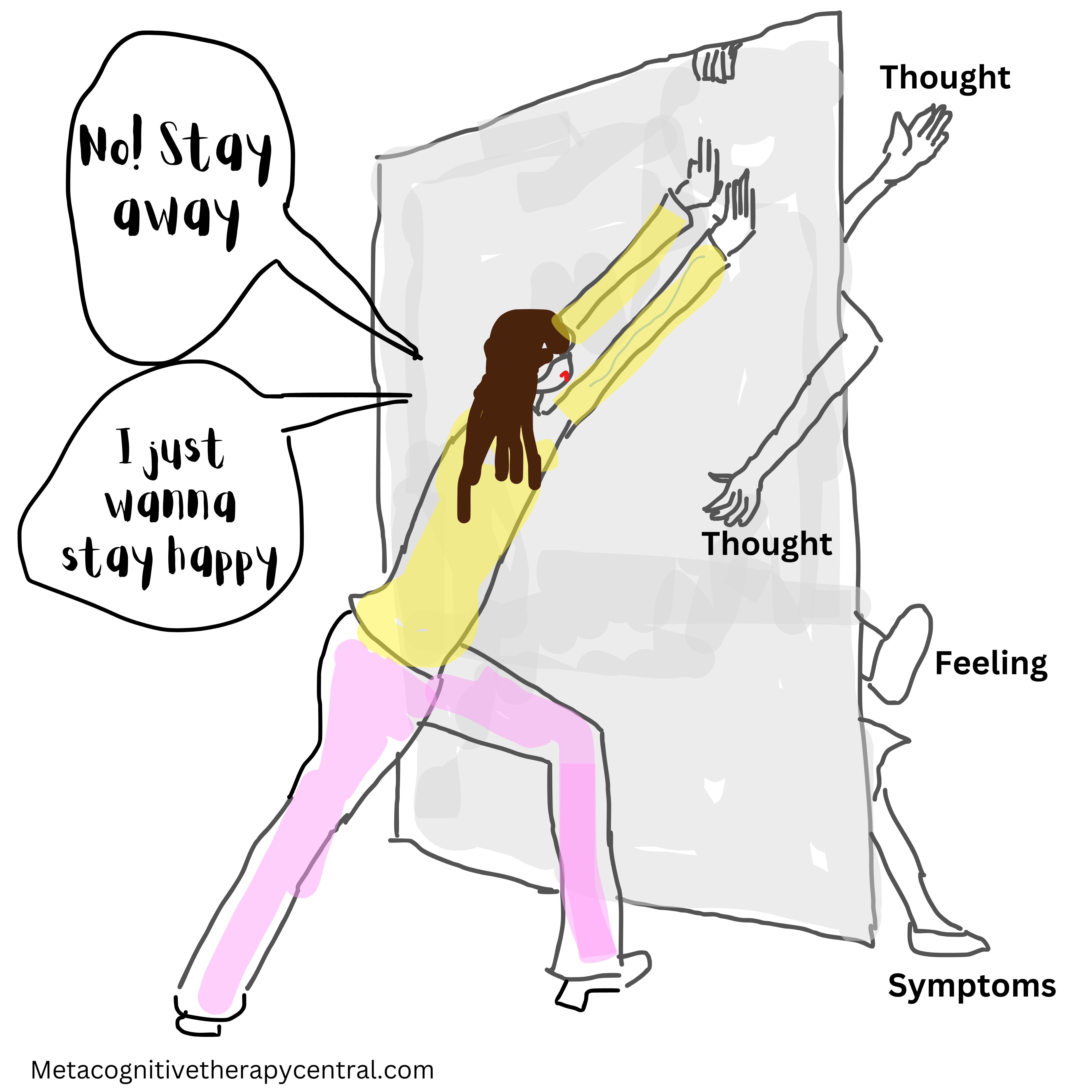
Context: This misconception arises because many of us have been taught that suppressing unwanted emotions isn’t beneficial. However, suppressing such emotions isn’t the same thing as applying detached mindfulness to our thoughts. Detached mindfulness is an important strategy in MCT. It is acknowledging an unwanted thought but choose to leave it alone (and let it exist and take up the space it wants).
Answer: The goal with detached mindfulness is to allow the mind to deal with unwanted thoughts on its own. But this critique highlights the importance of getting therapy from a skilled therapist who can help you understand detached mindfulness properly and set the right goals.
“If you can learn to control what thoughts you focus on, why not just focus on the positive thoughts instead?”
Context: It’s true that what you pay attention to tends to grow. If you dwell on your anxiety, it’s likely to increase. Similarly, if you constantly think about negative things, you’ll end up with more negative thoughts. So why not just focus on positive thoughts instead of negative ones?
Answer: But why exhaust yourself trying to focus solely on positive thoughts? It takes a lot of mental energy. Instead, why not focus on other important aspects of your life that automatically will help generate positive thoughts? It’s better and easier to practice not worrying or overanalyzing thoughts and trust that your mind will naturally gravitate towards more positive thoughts over time.

“CBT teaches the client new skills but that seems to be lacking in MCT”
Context: Learning skills is part of Cognitive-behavioral therapy (CBT). For example, CBT teaches you how to structure your day if you’re feeling depressed and demotivated, or how to behave in social situations if you’re socially anxious, or how to assert yourself and communicate better.
Answer: It’s true that MCT doesn’t focus on teaching specific skills like CBT does. The theory and the research behind MCT doesn’t support skills deficits as the reason behind mental illness. For example, if you have social anxiety, it’s not necessarily because you lack social skills. Research suggests that you might actually be too focused on yourself in social situations, which causes social anxiety (12).
Similarly, in Metacognitive couples therapy, clients often need little to no communication training. Once they learn to worry and ruminate less, they gain a clearer perspective on their problems and they can communicate better without extra training.
“Challenging metacognitive beliefs in a 6 weeks course group therapy is not enough time to really change them”
Context: In MCT, it’s important to not just worry less but also to change how we see our thoughts. For example, people with anxiety may think they can’t control their worrying, while those with OCD believe their thoughts are very important. These beliefs, called metacognitive beliefs, need to be challenged properly for MCT to really help.
Answer: I have led many MCT groups over the past four years, and in my experience, they’ve been effective at properly challenging metacognitive beliefs. However, achieving this depends on several factors:
A) What type of manual is used for the group therapy? Is it approved by the founder of MCT, and is there research supporting it?
B) How much do participants practice their new MCT strategies between sessions?
C) Is the therapist experienced?
D) How many participants are in the group session? (More in-depth discussions about each member’s challenges are possible in smaller groups, like six members compared to twelve.)
How to succeed with MCT
Criticism of Metacognitive therapy – your therapist’s opinion
Based on my experiences working with clients and discussions with my MCT colleagues, here are three main reasons why MCT may not be effective.
1. You are not ready to put in the work
Some people struggle with MCT because they don’t do the homework outside of sessions. This is a common reason why they don’t see improvements. In our experience, those who don’t practice or give up quickly often have a harder time benefitting from MCT.
MCT follows a specific structure outlined in a scientifically proven treatment manual. Clients are expected to practice them between sessions to get better. Therefore, doing MCT homework is really important for overcoming mental illnesses like anxiety and depression.
People who put in the effort to practice MCT usually see quick improvements in their mental health. The more they practice, the faster they get better. It’s not unusual for people to reduce excessive worrying in less than five sessions if they practice regularly.
In MCT, thoughts are viewed as part of the brain’s automatic system. While we may not always control them, we can decide how much attention we give to them
2. You don’t want to have negative thoughts or emotions
While it’s normal to want to push away negative thoughts, some people try really hard to get rid of them and expect therapy to help achieve this. In MCT, we teach that thoughts aren’t always accurate and aren’t that important. According to Professor Wells, who developed MCT, we can’t always control our thoughts because many just happen automatically (13). So, trying to directly control them is tough, but we can learn not to worry about them too much.
Wanting to completely erase negative thoughts is a tough goal, but many try it with MCT, even though it often doesn’t work well. Trying to get rid of thoughts is like suppressing them, which only makes anxiety worse. Instead, MCT teaches to spend less time worrying about negative thoughts and get better at it.
Suppression is the conscious process of pushing unwanted and uncomfortable thoughts and feelings out of the mind.
3. You want to ruminate and worry to solve problems
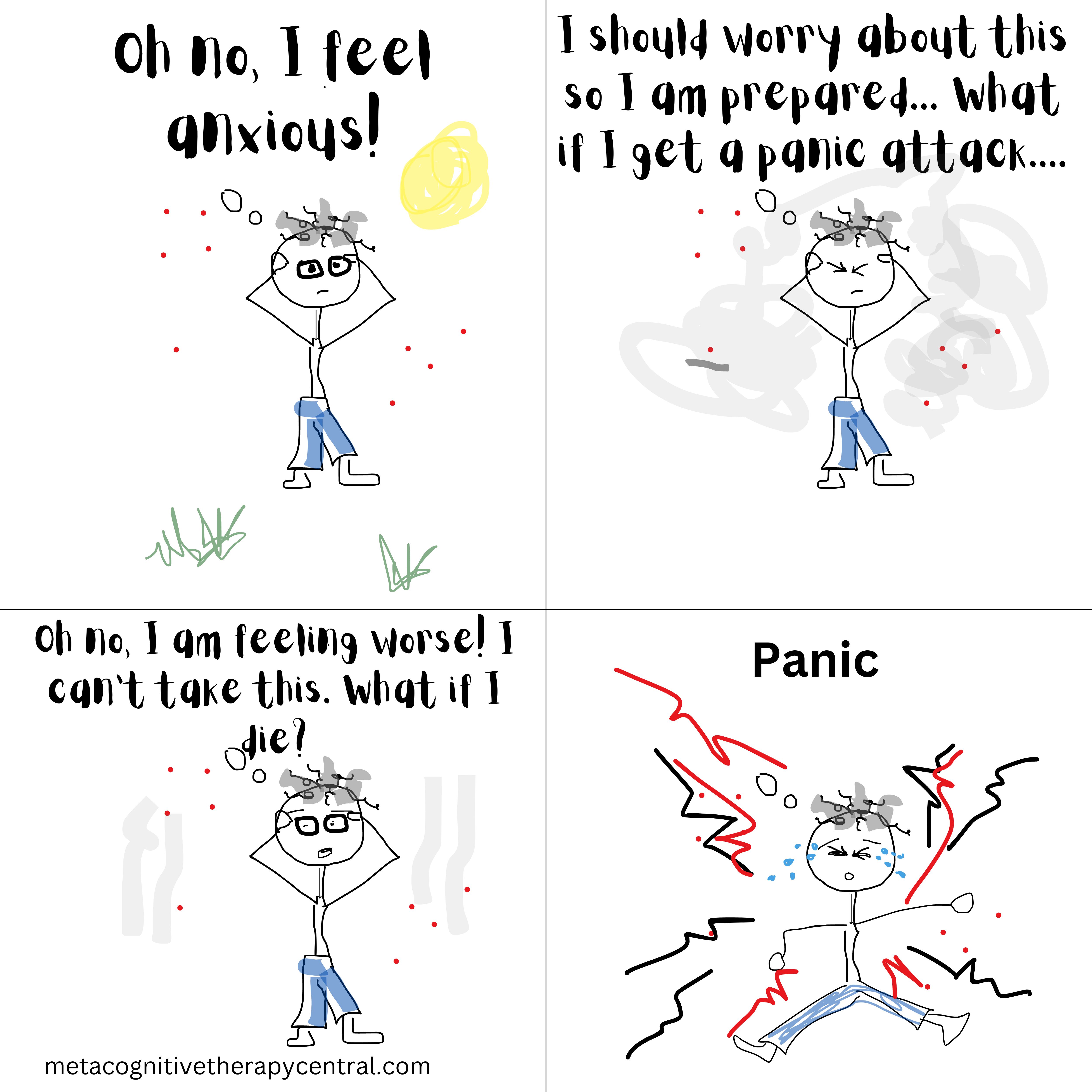
Some people think that constantly thinking about problems (rumination) or worrying about the future helps them solve problems or feel prepared. But according to MCT, rumination makes depression worse, and worrying fuels anxiety.
In MCT, we teach clients to control worry and rumination and use techniques like worry postponement. However, some people still struggle because they believe that worrying helps them stay in control or solve problems. For example, they might think that if they stop worrying, they won’t find good solutions to problems. Similarly, some with depression believe they need to keep thinking about what got them depressed to get better. These beliefs can make it hard for them to fully engage in therapy.
Will Metacognitive therapy still work for me?
While these factors can hinder progress in therapy, a skilled therapist can still work to challenge and change them. However, sometimes it’s just not the right time for therapy, but that might change in the future.
If you’re unsure whether any of these factors apply to you, book a free intro session and see whether MCT will be helpful for your specific problem.
References
- Moncrieff J, Cooper RE, Stockmann T, Amendola S, Hengartner MP, Horowitz MA. The serotonin theory of depression: a systematic umbrella review of the evidence. Mol Psychiatry. 2022:1–14.
- Jauhar, S., Arnone, D., Baldwin, D.S. et al. A leaky umbrella has little value: evidence clearly indicates the serotonin system is implicated in depression. Mol Psychiatry 28, 3149–3152 (2023). https://doi.org/10.1038/s41380-023-02095-y
- https://www.altinget.dk/artikel/psykologer-boern-med-angst-behandles-med-udokumenteret-terapiform
- Horvath, A. O., Del Re, A. C., Flückiger, C., and Symonds, D. (2011). Alliance in individual psychotherapy. Psychotherapy 48, 9–16. doi: 10.1037/a0022186
- Strauss AY, Huppert JD, Simpson HB, Foa EB. What matters more? Common or specific factors in cognitive behavioral therapy for OCD: Therapeutic alliance and expectations as predictors of treatment outcome. Behav Res Ther. 2018 Jun;105:43-51. doi: 10.1016/j.brat.2018.03.007. Epub 2018 Mar 27. PMID: 29621650; PMCID: PMC5939572.
- Schweiger JI, Kahl KG, Klein JP, Sipos V and Schweiger U (2019) Innovation in Psychotherapy, Challenges, and Opportunities: An Opinion Paper. Front. Psychol. 10:495. doi: 10.3389/fpsyg.2019.00495
- Solem, S., Wells, A., Kennair, L. E. O., Hagen, R., Nordahl, H., & Hjemdal, O. (2021). Metacognitive therapy versus cognitive–behavioral therapy in adults with generalized anxiety disorder: A 9‐year follow‐up study. Brain and Behavior, 11(10), e2358.
- Solem, S., Kennair, L. E. O., Hagen, R., Havnen, A., Nordahl, H. M., Wells, A., & Hjemdal, O. (2019). Metacognitive therapy for depression: A 3-year follow-up study assessing recovery, relapse, work force participation, and quality of life. Frontiers in Psychology, 10, 2908.
- Johnsen, T. J., & Friborg, O. (2015). The effects of cognitive behavioral therapy as an anti-depressive treatment is falling: A meta-analysis. Psychological Bulletin, 141(4), 747–768. https://doi.org/10.1037/bul0000015
- Normann, N., & Morina, N. (2018). The efficacy of metacognitive therapy: A systematic review and meta-analysis. Frontiers in Psychology, 9, Article 2211. https://doi.org/10.3389/fpsyg.2018.02211
- Sharma, V., Sagar, R., Kaloiya, G., & Mehta, M. (2022). The scope of metacognitive therapy in the treatment of psychiatric disorders. Cureus, 14(3)
- Leigh E, Chiu K, Clark DM (2021) Self-focuse attention and safety behaviours maintain social anxiety in adolescents: An experimental study. PLoS ONE 16(2): e0247703. https://doi.org/10.1371/journal.pone.0247703
- Wells, A., personal communication, 2022.