Metacognitive therapy is the best approach I have ever practiced with clients. Not only does its premise make logical sense (spending too much time thinking about negative stuff makes you feel bad), it treats emotional difficulties faster than any other approach I have come across (some clients recover from anxiety in under 5 sessions!).
Metacognitive therapy (MCT) differs from CBT by reducing the time spent overthinking problems, not problem content. To reduce overthinking, it’s important to believe that you can control it. MCT teaches you to rediscover this control.
This post will help you understand the important points about MCT and provide you with answers to commonly asked questions.
What is Metacognitive therapy?
MCT is a psychotherapy (talk therapy as a mental health treatment). It’s based on solid ideas about why people feel anxious or depressed, and scientists, including the founder of MCT, Professor Wells, have been studying it for over 25 years. Recent studies show that it’s really good at helping with various mental health issues, and even experts recommend it for social anxiety (1).
Now, what makes a mental health treatment reliable and effective?
According to researchers (2), it is important that the treatment clearly points out:
- What makes us mentally ill (anxiety, depression, OCD, PTSD, etc.)
- How exactly does this treatment treat mental illness
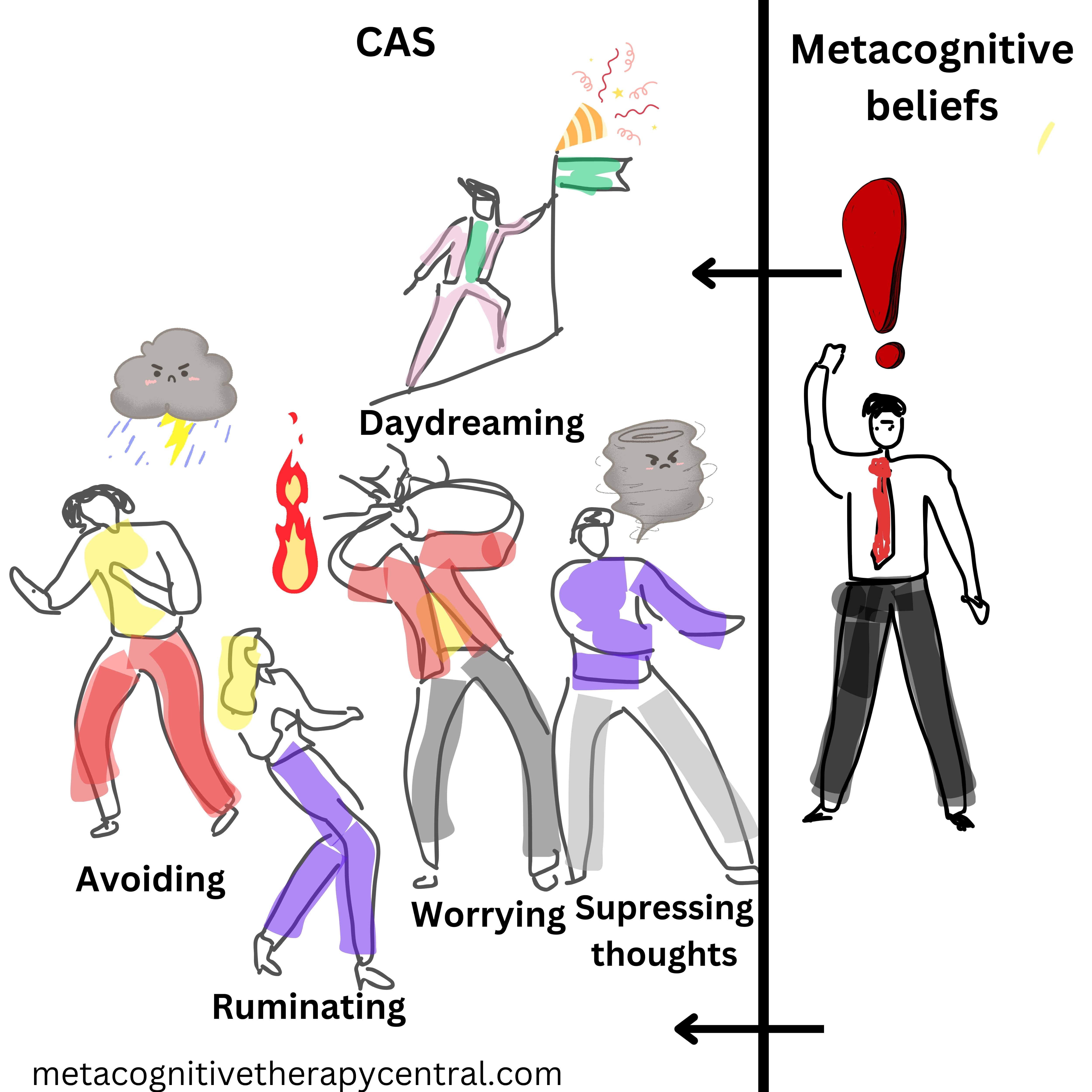
In MCT, a specific unhelpful thinking style (called CAS) and beliefs about thinking (called metacognitive beliefs) cause mental illnesses. So to recover from, for example, anxiety disorder, MCT helps you reduce the CAS and change false beliefs about your thinking.
MCT can help us leave negative thoughts and feelings alone (instead of worrying about them) so that the mind can self-regulate.
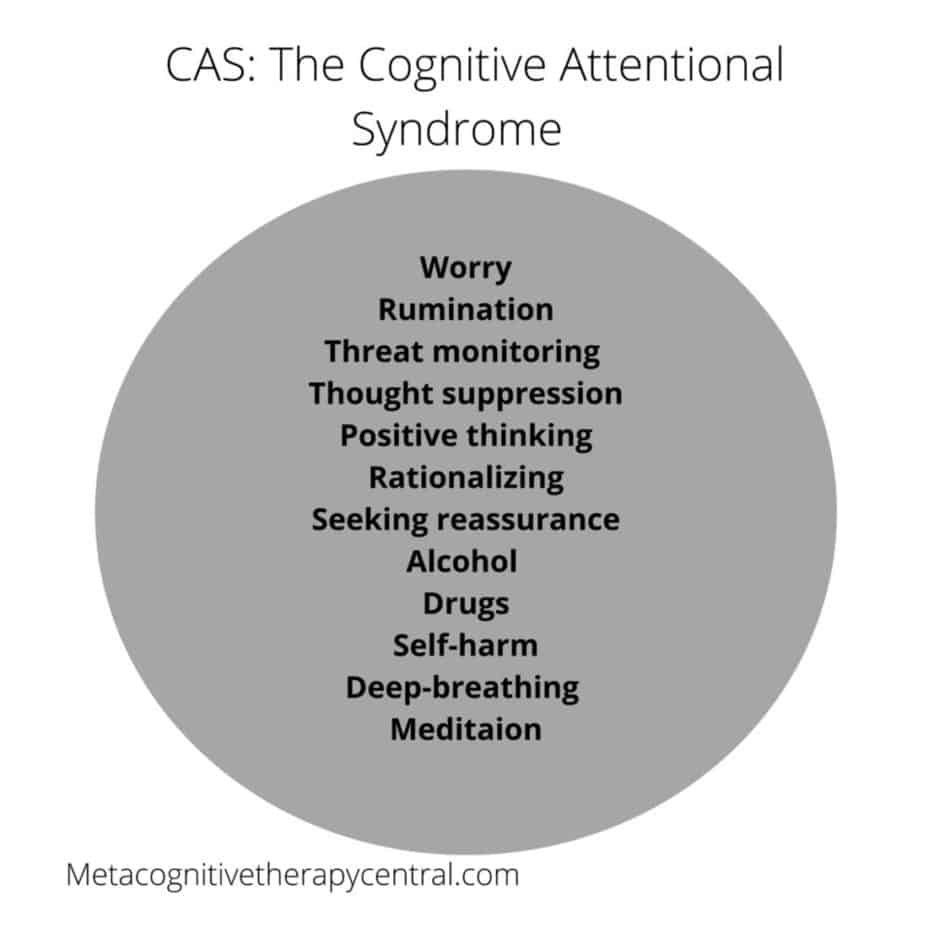
What is CAS?
CAS stands for the cognitive attentional syndrome and consists of
- Worrying/ruminating
- Paying attention to threats
- Other coping strategies (avoiding difficult situations/emotions, suppressing thoughts, seeking reassurance, taking substances)
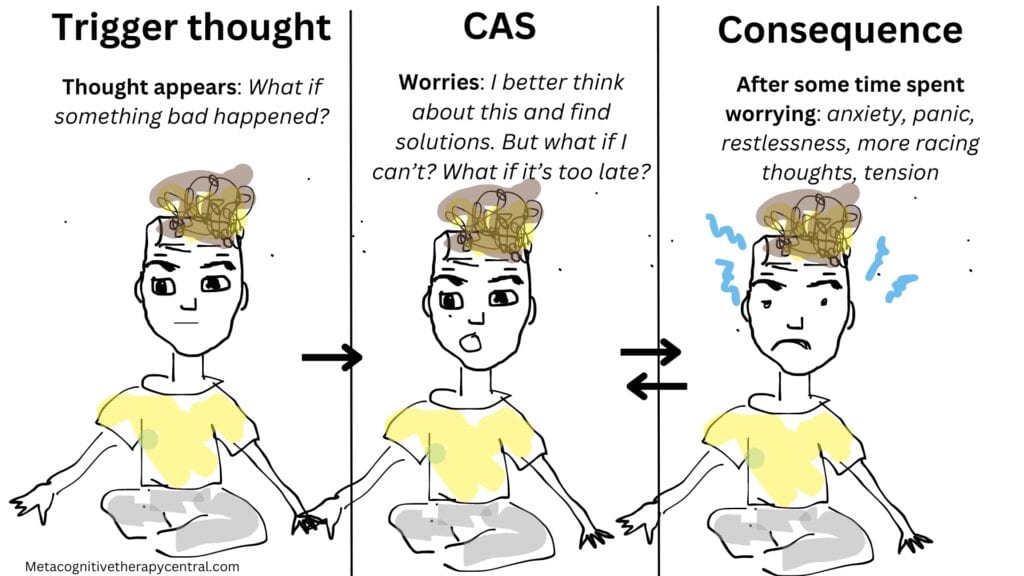
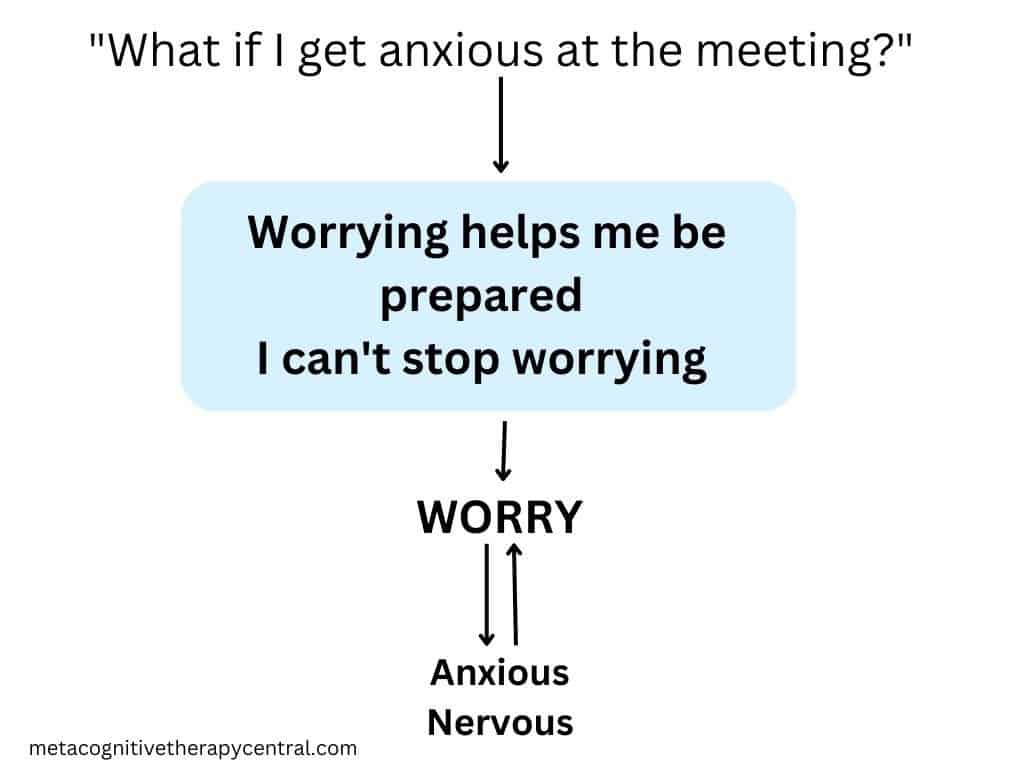
The CAS, done for a long time, is what makes us feel anxious, stressed, or depressed. For example, imagine if you spent hours worrying about, “What if I mess up the presentation tomorrow?“, you would feel pretty stressed out and nervous by the end of the day.
What is self-regulation?
Dwelling on negative thoughts/emotions and problems impacts the mood negatively because of the way the brain works. The theory behind MCT shows that the mind can self-regulate (3). This is similar to how the body can heal itself from wounds and cuts, the mind can also heal itself from negative thoughts, feelings, and stressful experiences.
Having negative thoughts and feelings is normal and these thoughts and feelings are momentary. The mind will take care of them if we leave them alone.
Self-regulation is when your mind allows thoughts and feelings to flow through without getting stuck. Whatever comes up in the mind will pass through, just like sand slipping through the holes in a sieve.
However, the CAS will prevent self-regulation from happening and thereby make unwanted thoughts and feelings linger for a longer time. This is why we develop mental illness according to MCT (5).

What are metacognitive beliefs?
The reason why people ruminate in the first place is because of their metacognitive beliefs, which are beliefs and plans about how we think (4). Examples of metacognitive beliefs are, I need to ruminate to solve problems, and I can’t stop ruminating.
Imagine metacognitive beliefs as the captains of our thinking process. They are the big beliefs that control how we handle thoughts, for example through overthinking or worrying, and the tactics we use to avoid feeling uncomfortable.
For example, having the belief I can’t control my thoughts is called an uncontrollability belief, while believing Worrying is harmful to my body is called a danger belief. There are also beliefs like If I worry, I’ll be prepared or Rumination helps me understand my problems. These are called positive beliefs.
In some cases, especially with conditions like OCD or psychosis, people have beliefs about how important their thoughts are. They believe If I have a thought, it must be true, or Outside forces can put thoughts in my head.
Beliefs about our thinking shape how we navigate and deal with our thoughts, but just because we believe them, they are not necessarily accurate. For example, with the right strategies, we can always control how much we worry.
How do metacognitive beliefs affect mental health?
Rumination and worry are activated by metacognitive beliefs.
According to metacognitive therapy, negative metacognitive beliefs prevent healthy emotion regulation and create psychological illness.
The mind can self-regulate negative thoughts and feelings, but this process gets interrupted by rumination and worry.
When we don’t believe in our ability to control rumination and worry, we will continue to worry and ruminate for a long time whenever we have unwanted thoughts or feelings. But worrying/ruminating (dwelling and chewing on our thoughts) interrupts self-regulation and maintains how sad/anxious/angry/hopeless we feel.
But although excessive rumination/worry causes mental illness, these thinking styles are not harmful. For example, worrying can’t make you go mad or damage your body. Rumination can’t damage your brain.
Experiment: Measure your mood on a scale from 0 (terrible) to 10 (amazing). Then try to think of something that upsets you and decide to think about it for 2 minutes. Measure your mood again from 0-10. How did dwelling on your thoughts impact your mood?
How does metacognitive therapy work?
MCT helps you reduce the CAS and change metacognitive beliefs so that your mind can get back to self-regulating. This is not a quick fix, but so far, it is the fastest and most effective way to recover from chronically feeling down, anxious, panicky, or stressed.
This happens through teaching you to leave your upsetting thoughts alone and postpone worrying about them until later. Some of the techniques used in therapy are:
- detached mindfulness (acknowledge that you have a negative thought in your mind that fights for your attention, but decide not to deal with it)
- worry postponement (postpone worrying/ruminating for your 30-minute worry time later in the day)
- challenging metacognitive beliefs (your therapist will help you challenge these beliefs by doing experiments to test whether they are accurate)
Example of detached mindfulness
A common metaphor for detached mindfulness is the running sushi. It illustrates the natural flow of thoughts, similar to plates of sushi moving towards and away from you in a running sushi restaurant.
When practicing detached mindfulness, I ask my clients to observe their unwanted thoughts come and go the same way they would observe the sushi plates on the conveyor belt. This exercise emphasizes their ability to choose whether or not to engage with their thoughts.
Experiment: Imagine looking at plates of sushi on a conveyor belt, moving towards and away from you. Just watch them come and go without grabbing every plate. In a similar way, you can observe your thoughts come and go in your mind.
I have covered everything you need to know about detached mindfulness here.
Read: Does metacognitive therapy work and how?
What is metacognitive therapy good for?
MCT is good for treating mental disorders that are caused by negative thinking styles like worry and rumination. For example, MCT has proven to effectively treat anxiety disorders (Generalized anxiety disorder, panic disorder, health anxiety, social anxiety), PTSD, OCD, and depression.
| Mental health issue | How MCT treats it |
| Anxiety | Learn to reduce worrying Trust your ability to stop worrying without distracting yourself or seeking reassurance Learn that worrying/anxiety is not harmful |
| Social anxiety | Learn to reduce worrying about how you come across Learn to reduce analyzing your social interactions Control your ability to focus outside of yourself |
| OCD | Learn not to respond to intrusive thoughts (instead of worry/rumination/performing rituals) Understand that thoughts don’t make things happen in the external world Develop a relaxed relationship with intrusive thoughts |
| Depression | Become aware of and reduce how much time you spend ruminating Develop a relaxed relationship with depressive thoughts and emotions Learn to focus attention outside of your thoughts |
How do you do Metacognitive therapy compared to other treatments?
MCT is unique compared to other treatments because of what it thinks causes mental illness. According to MCT, it is not what we think but how we think that makes us feel bad.
For example, Cognitive-behavioral therapy (CBT) believes that the content of thoughts (negative automatic thoughts, e.g. what we think) leads to mental disorders like anxiety and depression. CBT, therefore, treats depression/anxiety by challenging the content and the validity of thoughts (“I am hopeless” or “What if I get a heart attack?“): What is your proof that you will get a heart attack?
Metacognitive therapy is not interested in the content of thoughts. Instead, an MCT therapist is interested in how people deal with their unwanted thoughts. Do they worry about these thoughts or try to push them away? Once the client’s unhelpful strategies are identified, the therapist works collaboratively with the client to reduce these unhelpful strategies and change false beliefs about thinking that may get in the way.
MCT is different from other psychological interventions because it doesn’t try to change thoughts and feelings. Instead, it focuses on reducing how much time we spend overthinking by showing us that we can control this process.
Essentially, this is one of the most important points my clients learn after MCT:
I can’t control what thoughts I get. But I can choose not to respond to them by worrying .
What are the goals of Metacognitive therapy?
The goals of MCT are to identify the processes that maintain mental illness and help you recover by:
- Developing a relaxed relationship with thoughts/emotions
- Understanding that you have full control over how you deal with thoughts/emotions
- Reducing the time you spend worrying/analyzing thoughts
An MCT therapist will ask very direct questions and do thinking experiments with their clients.
For example, some of my clients believe that they can lose control and go crazy from having negative thoughts. I therefore ask them to try to lose control over themselves by worrying intensely about these thoughts in the session.
Other clients believe that thinking bad thoughts will make them do bad things. So I ask them to think intensely about these bad thoughts and see if their thoughts alone affect reality.
Of course, neither feared outcome comes true, and this helps change my clients’ false beliefs about how their thinking works.

Below is an example of a metacognitive intervention.
An MCT therapist will ask her patients some of the following questions (based on Wells’s manual for treating depression): (4)
“How effective has your rumination been in getting rid of your depression?“
“You believe that rumination helps to solve your depression. How much do you believe that?“
“Let’s practice a different way of responding to the thoughts or feelings that act as triggers for ruminating.
“When you notice a negative thought, you can say to yourself: “There is a negative thought. I’m not going to deal with it now; I am not going to activate my rumination.”
Overthinking and holding onto wrong ideas about thoughts can cause and maintain mental health challenges. When you learn to cut down on overthinking, it helps your mind deal with emotions faster and supports a quicker recovery.
Is metacognitive therapy evidence-based?
This systematic review and meta-analysis of randomized trials (measuring the effect of MCT based on many independent studies) for anxiety and depression shows that MCT is very effective.
MCT not only reduces symptoms of anxiety and depression but also other symptoms like insomnia and relationship difficulties for example. The effect is also greater than for cognitive-behavioral therapies and is supported by this and this study.
Evidence for the theory behind Metacognitive therapy
The theory behind MCT (the S-REF) (4) (5) describes how mental illness is caused:
- Most mental disorders are caused by a common factor which is negative thinking (overthinking) that is extensive and difficult to control.
- Psychological distress can recover (self-correct), but it is prevented by overthinking and other unhelpful (maladaptive) coping strategies.
- Metacognitions (metacognitive beliefs) play a critical role when it comes to psychological illness and when it comes to psychological resilience.
Here is some of the research about the S-REF:
This study shows that metacognitive beliefs about worry predict anxiety in people. It seems that false metacognitive beliefs create psychological vulnerability in people in the first place.
This study finds that metacognitive beliefs predict whether people get anxiety and how anxiety affects metacognitive beliefs.
This study examines the effects of worry about worry (meta-worry) and resilience when performing complex tasks. The participants in the study who worried about their worrying experienced more stress and had a harder time adapting to the stress.
This study demonstrates that when 7-14 year-olds believed less in controlling their attention, the more anxiety symptoms they reported. On the other hand, 7-14 year-olds who believed in their ability to control their attention did not get anxious despite having dysfunctional metacognitive beliefs. This study proves that there is a close relationship between metacognitive beliefs, attention control, and anxiety.
This study validates how the CAS disrupts emotion regulation in the brain. The effect of CAS was tested on neural connections in the brain using fMRI during negative thinking.
If you want to know more about the research behind MCT, read this post.
What is the success rate of MCT?
According to recent research, MCT’s success rate in treating anxiety is 72% (7), and 74% (6) for depression.
My experience in working with clients is that those who consistently practice what they learn in therapy are successful in achieving good outcomes. However, some clients still choose to want to get rid of unwanted thoughts and emotions, and their progress may therefore be slower.
How is metacognitive therapy different from CBT?
Metacognitive therapy is not CBT because CBT links mental disorders to the content of thoughts, while MCT links mental disorders to unhelpful and extended thinking styles (CAS) and metacognitive beliefs.
Both approaches think that a higher-order system controls thinking, but in CBT, these consist of beliefs about oneself or the world, while in MCT, they consist of beliefs about thinking itself (metacognitive beliefs).
CBT: what your thoughts say causes mental illness. MCT: how you think about your thinking causes mental illness
Is MCT better than CBT?
Research proves that CBT has a 50% recovery rate. MCT targets the parts of thinking that treat mental disorders more effectively, with a 70% recovery rate and fewer cases of relapse (6) (7).
Adrian Wells (the founder of Metacognitive therapy) argues that the content of thoughts doesn’t lead to emotional disorders by themselves. After all, people can choose how they respond to thoughts like “I am a failure” and get different outcomes. If they dwell on the thought, they could become depressed, but if they leave it alone, they will be unaffected by it (4).
There seems to be a missing link between having a negative thought and feeling depressed. CBT is not able to explain that link. Metacognitive therapy can do that and the answer is metacognitive beliefs.

Research on CBT vs. MCT
A study from 2015 tested whether schemas (CBT beliefs about oneself, other people, and the world) or metacognitive beliefs contribute to depression.
The researchers recruited participants and had them fill out questionnaires about metacognitive beliefs and depressive schemas.
MCT – Examples of metacognitive beliefs questions were:
“I cannot stop myself from ruminating”
“Ruminating makes me physically ill”
“People will reject me if I ruminate”
“Ruminating about the past helps me to prevent future mistakes and failures”
CBT – Examples of depressive schemas were :
“My life is wasted unless I am a success”
“If others dislike you, you cannot be happy”
“What other people think about me is very important”
“I should be happy all the time”
The results of the study were clear: the more people were convinced of their metacognitive belief, the more depressed they felt. On the contrary, the CBT schemas were not associated with depressive symptoms, making metacognitive therapy a better theoretically founded therapy for mental disorders compared to CBT.
Is MCT or CBT better at treating generalized anxiety disorder? Read this post.
What are the disadvantages of Metacognitive therapy?
So far, there are no known scientifically proven disadvantages of MCT. Rather, there might be fewer downsides to MCT compared to other therapies that delve into negative thoughts and traumatic experiences (for example, psychoanalytic approaches).
However, there is criticism of MCT that it is mainly researched by the same people who founded it. Many of the larger studies that prove the effect of MCT are also conducted by Professor Wells, the founder of MCT, although many of those are of high quality.
There is a need for independent researchers to also look into the effect of MCT in the future and larger studies of MCT across different populations.
Summary
- MCT is well-researched and it is proven to work for mental illnesses like anxiety and depression amongst others
- MCT’s theory (S-REF) explains how metacognition (beliefs about thoughts and how we think) is more important in causing mental illness than the content of thoughts themselves
- MCT has proven to be better at treating anxiety and depression than cognitive-behavioral therapy (CBT)
- There are currently no known disadvantages of MCT, and the recovery rate is at 70-80%
References
- NCCMH (2013). Social anxiety disorder: the NICE guideline on recognition, assessment and treatment. Leicester & London: The British Psychological Society and the Royal College of Psychiatrists (Full Guideline). https://www.nice.org.uk/guidance/cg159/chapter/Recommendations#interventions-for-adults-with-social-anxiety-disorder-2
- Schweiger JI, Kahl KG, Klein JP, Sipos V and Schweiger U (2019) Innovation in Psychotherapy, Challenges, and Opportunities: An Opinion Paper Front. Psychol. 10:495. doi: 10.3389/fpsyg.2019.00495
- Wells A (2019) Breaking the Cybernetic Code: Understanding and Treating the Human Metacognitive Control System to Enhance Mental Health. Front. Psychol. 10:2621. doi: 10.3389/fpsyg.2019.02621
- Wells, A. (2009). Metacognitive therapy for anxiety and depression. Guilford Press.
- Wells, A., & Matthews, G. (1996). Modelling cognition in emotional disorder: The S-REF model. Behaviour Research and Therapy, 34(11-12), 881–888. https://doi.org/10.1016/S0005-7967(96)00050-2
- Callesen, P., Reeves, D., Heal, C. et al. Metacognitive Therapy versus Cognitive Behaviour Therapy in Adults with Major Depression: A Parallel Single-Blind Randomised Trial. Sci Rep 10, 7878 (2020). https://doi.org/10.1038/s41598-020-64577-1
- Nordahl HM, Borkovec TD, Hagen R, Kennair LEO, Hjemdal O, Solem S, Hansen B, Haseth S, Wells A. Metacognitive therapy versus cognitive-behavioural therapy in adults with generalised anxiety disorder. BJPsych Open. 2018 Sep 11;4(5):393-400. doi: 10.1192/bjo.2018.54. PMID: 30294448; PMCID: PMC6171331.