
Metacognitive therapy works very well for treating anxiety disorder, depression, post-traumatic stress disorder, obsessive-compulsive disorder, and psychosis.
Metacognitive therapy (MCT) is a science-backed psychotherapy approach attributing mental illness to unhelpful thinking patterns like excessive rumination and worry. MCT aims to reduce these thinking styles and change the metacognitive beliefs that activate them.
Several published studies have tested the effects of MCT, which is recommended as an evidence-based treatment option for anxiety in the UK. The success of Metacognitive therapy is due to the discovery of the self-regulating mechanism in the brain.
Why does MCT work?
New theories about thinking helps us understand how MCT works. Adrian Wells’ 2019 theory, the Metacognitive Control System (MCS), explains two thinking systems in our brain: MCS (metacognitive knowledge) and CS (where thinking happens).
According to Wells, the mind can self-regulate and heal itself from psychological wounds, negative thoughts and emotions, provided that the metacognitive beliefs in the MCS are aligned with this goal.
If the metacognitive beliefs instead promote worry and rumination, they will hinder self-regulation and contribute to mental illness.
This theory crucially explains the origin of mental illness (blocked self-regulation due to excessive rumination and worry) and outlines an effective treatment approach (reducing rumination, worry, (and other unhelpful thinking styles) and reshaping metacognitive beliefs).
According to MCT theory, the mind can heal itself from various mental disorders provided that unhelpful thinking patterns are reduced.
MCT has a clear theoretical foundation
Most existing therapies are built on a combination of techniques which makes it difficult to understand how they really work in treating mental illness. For example, Cognitive-behavioral therapy (CBT), which is the most scientifically acknowledged therapy for anxiety and depression in the last 40 years, only has a 50% improvement rate. And this effect seems to get worse over time (1).
There is a need for a more precise theoretical foundation for therapy to better help people recover from mental illness. Metacognitive therapy, (MCT), is an example of this type of approach. It is based on a comprehensive theory explaining exactly why people become mentally ill, and it offers a solution that works across various disorders with good effect (2).

Is MCT better than other treatments?
Research shows that Metacognitive therapy works better than CBT for depression and anxiety, better than Eye Movement Desensitization and Reprocessing (EMDR), for Post-traumatic stress disorder, and better than Dialectical Behavior therapy (DBT), for treating Borderline personality disorder, which is traditionally known as a difficult disorder to treat (3).
| Recovered with MCT | Recovered with CBT | |
| Anxiety Study by Nordahl et. al 2018 Study by Solem et. al 2021 | 65% 57% + 14% | 38% 38% + 25 % |
| Depression Study by Callesen 2020 | 74 % | 56 % |
| OCD Study by Papageorgiou et. al 2018 | 86,3 % responded to treatment | 64 % responded to treatment |
What is MCT?
Metacognitive therapy is developed by clinical psychologist and professor Adrian Wells. MCT has almost 30 years of clinical research backing up its theoretical foundation and clinical impact on mental health disorders (4).
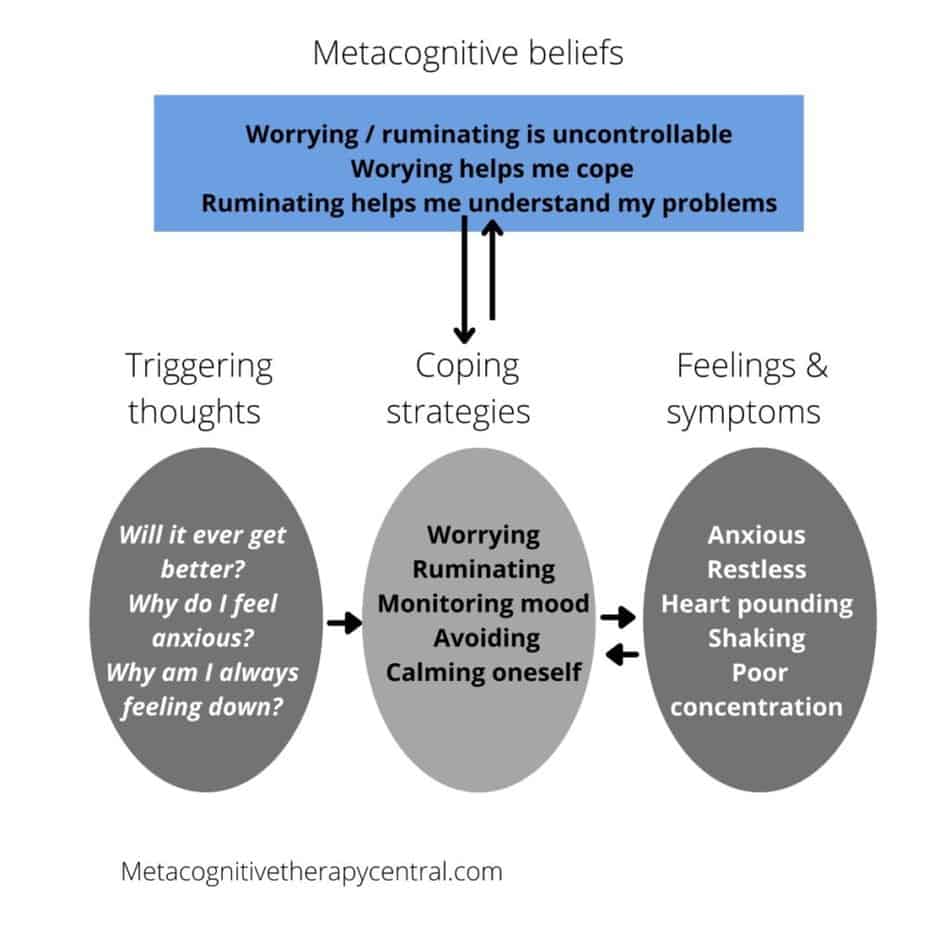
According to Metacognitive Therapy, most psychological disorders develop from unhelpful coping strategies like rumination and worry and from metacognitive beliefs.
Metacognitive beliefs are beliefs about the way we think. For example, most people with mental illness have the following metacognitive beliefs “Worry is uncontrollable” or “I need to worry to feel better.” This makes them start worrying about negative thoughts, which in turn makes them feel more anxious. But because they don’t believe that worrying can be stopped, they start using different strategies to control worry.
The unhelpful coping strategies are called the Cognitive attentional syndrome, CAS, consisting mainly of rumination and worry, but also thought suppression, monitoring for threats, avoidance, and reassurance seeking.
What is mental illness according to Metacognitive therapy?
Metacognitive beliefs and CAS play an important role in whether we get mentally ill. This happens because metacognitive beliefs tell us to worry, ruminate, or suppress negative thoughts. In other words, Metacognitive beliefs activate the CAS, and CAS will inevitably make us feel anxious, depressed, and stressed.
How does MCT work?
MCT reduces rumination and worry through strategies like called Detached mindfulness and worry postponement, and by changing metacognitive beliefs.
Detached mindfulness means observing thoughts and feelings in a detached way, without engaging or suppressing them. This allows the mind to heal itself from negative thoughts and feelings, which is an ability that everyone naturally has.
Worry postponement has the goal of reducing the daily time spent worrying by postponing worry to a daily fixed time window.
Aside from reducing overthinking, an important part of why MCT works is because it effectively changes metacognitive beliefs. When metacognitive beliefs are biased they don’t allow the mind to self-regulate and take care of the negative thoughts and emotions.
Metacognitive beliefs are biased when we interpret thoughts and feelings as dangerous and believe that overthinking can’t be stopped.
Metacognitive beliefs are like the lenses we view our inner world. If they are clear and accurate, we see thought and feelings for what they are: brief and harmless. But if they are foggy or distorted, our thoughts, feelings, and thinking seem like a threat to us. Think of MCT like cleaning the foggy lens.
MCT helps the mind heal itself
Much like the body’s ability to heal a broken bone, the mind can heal itself from feeling down or anxious.
Thoughts, images, and urges visit the conscious part of the brain shortly but will disappear again on their own. However, if we grab on to the thoughts and ruminate and worry about them, they will stay much longer.
If we grab on to unwanted thoughts and feelings, we hinder the mind from regulating itself. And that’s when thoughts and feelings stay in the mind for a longer time, causing mental disorders like anxiety, depression, PTSD, and other mental issues.
But, if we leave these thoughts and images alone, they will pass through like grains of sand in a strainer.
How do you do MCT?

Metacognitive therapy treatment is manualized, meaning that the therapist follows a specific guide to lead the sessions. However, the therapist always aims to tailor the treatment to the patient’s particular needs.
Here are the general MCT treatment steps (5) that MCT therapists follow, based on the work of Adrian Wells. The combination of the techniques will vary depending on the patient.
First step: Explain how the patient’s specific strategies like worry and rumination maintain their mental illness.
Second Step: Help the patient realize that their coping strategies are ineffective in solving problems.
Third Step: Identify the patient’s metacognitive beliefs and challenge them through experiments. For example, almost all patients have metacognitive beliefs about not being able to control worry and ruminations. This is called an uncontrollability belief, and as long as this is prominent, the patient won’t try to stop worrying despite the anxiety that worrying creates.
Metacognitive beliefs are tested and challenged in almost every session, so they gradually change throughout therapy.
Unchanged metacognitive beliefs are why people relapse into mental illness after therapy, despite having reduced their symptoms. Therefore, metacognitive beliefs are extremely important to address in MCT.
Fourth Step: The patient learns to postpone worry and rumination in therapy and for homework. This will help them realize that worry and rumination are harmless and have no advantages.
Fifth Step: The patient learns attention training technique and detached mindfulness to gain flexible attention. Flexible attention will help to focus attention away from negative thoughts and toward meaningful activities. That allows the mind to self-regulate from negative thoughts and feelings and with time recover from mental illnesses.
Through detached mindfulness, the patient learns to become aware of negative thoughts and detach from them by taking a step back and discontinuing worry and rumination.
Homework: The patient practices detached mindfulness between sessions. This strengthens the patient’s ability to stop worry and rumination and enhances the belief that worry and rumination are controllable.
Toward the end of therapy, the focus is on reversing any residual coping strategies like avoidance, reassurance-seeking, and positive thinking, and preventing relapse into mental illness.
Free MCT E-book
Organize your MCT exercises and learn how to use them to reduce worry and rumination. Download free e-book here.
Evidence for MCT – five important research findings
The scientific data supporting the theory and practice of MCT is only growing. Below, you can read about some of the largest and most recent studies on Metacognitive therapy.
1) Proof of metacognitive theory
“Breaking the Cybernetic Code: Understanding and Treating the Human Metacognitive Control System to Enhance Mental Health”
What is it about?
This paper (6) is written by the originator of Metacognitive therapy, Adrian wells. Wells describes the theory behind MCT through the interaction in the metacognitive system in the brain; a mechanism called the “cybernetic code” which is metacognitive information.
What did they find?
The cybernetic code is a code sent in the brain that leads to feeling distressed. The code is short and leads to emotional recovery on its own, which means that uncomfortable feelings naturally don’t last long in the human mind. However, the code is prolonged and extended by the use of unhelpful coping strategies, which means that uncomfortable feelings will last longer in the mind.
What do the findings mean?
This finding is revolutionary because it explains that negative thoughts and feelings are temporary. Feelings of anxiety, sadness, and stress are brief in nature. But when a person responds to these with the activation of the CAS (worry, rumination, and thought suppression), they cause increased psychological distress and may unintentionally exacerbate and prolong anxiety and depression.
It seems that getting mentally ill is something that we can learn to control. The future implications of the science behind MCT can be huge, scientifically, economically, and politically.
2) Review of 25 largest MCT studies
“The Efficacy of Metacognitive Therapy: A Systematic Review and Meta-Analysis”
What is it about?
Researchers from Denmark and Germany analyzed the combined results of 25 scientific studies on Metacognitive therapy. They did this through statistics because they wanted to make an updated study of the effect of Metacognitive therapy on different psychological issues like anxiety, depression, PTSD, and grief (7).
Who participated?
The psychological issues that were treated through MCT were depression, bipolar II disorder, generalized anxiety disorder, post-traumatic stress disorder, cancer distress, schizophrenia spectrum disorders, body dysmorphic disorder, hyposexual desire disorder, obsessive-compulsive disorder, and grief.
468 patients were analyzed in total. Some of these patients received MCT and were compared to the rest of the patients that were on a waiting list and not receiving MCT.
What did they find?
The results from before and after treatment and follow-up (usually follow-up testing is done 6 to 12 months after treatment) suggest that MCT effectively reduces psychological issues, including anxiety, depression, as well as dysfunctional metacognitive beliefs. The researchers also found indications that Metacognitive therapy could be more effective than other therapies.
What do the findings mean?
The findings mean that Metacognitive therapy is an effective treatment for psychological disorders. MCT may also become an alternative to Cognitive-behavioral therapy (CBT). Cognitive-behavioral therapy is well researched, but the effect on treating psychological disorders is dropping.
Metacognitive therapy can someday become a faster and more cost-effective alternative treatment for mental disorders.
3) Comparing MCT with CBT for anxiety
“Metacognitive therapy versus cognitive–behavioural therapy in adults with generalised anxiety disorder”
What is it about?
Researchers (8) from Norway compared MCT with CBT in patients with generalized anxiety disorder. CBT is known as one of the most researched therapies and the best choice for anxiety.
Who Participated?
Eighty-one patients with generalized anxiety disorder were divided into three conditions: 28 were treated with CBT, 32 with MCT, and 21 were on a waiting list and received no treatment.
The therapists were crossed over halfway through the study to make sure they did not affect the results in any way. Each therapist treated half the patients with CBT and the other half with MCT.
What did they find?
The results from before and after treatment and at two-year follow-up showed that both CBT and MCT effectively treated anxiety. But MCT was more effective than CBT (65% v. 38%).
What do the results mean?
Anxiety patients recover better when they are treated with MCT than CBT. They also stay recovered two years after treatment. MCT is effective, fast, and prevents relapse back into anxiety.
Note: a recent study(9) following up on the effects of MCT compared with CBT for anxiety disorders after 9 years shows similar results. More patients recover and stay recovered 9 years after treatment with Metacognitive therapy compared to CBT. Read about the study here.
4) Comparing MCT with CBT for Depression
“Metacognitive Therapy versus Cognitive Behaviour Therapy in Adults with Major Depression: A Parallel Single-Blind Randomised Trial”
What is it about?
Danish psychologist Pia Callesen assessed the effectiveness of MCT compared to CBT in adults with major depressive disorder (10).
Who Participated?
172 adults with major depressive disorder were randomly divided so that 85 patients received MCT and 89 received CBT.
The participants did not know if they were receiving the real treatment or a placebo. This was done to reduce any risk of errors. Each group received up to 24 sessions of therapy by trained clinical psychologists.
What did they find?
74% of the patients who received MCT recovered from depression compared with 52% of the patients who received CBT.
The results were the same six months after treatment (MCT 74% and CBT 56%). Usually, a 50% recovery rate is good for CBT.
The patients not only recovered from depression, but they also improved their metacognitive beliefs (beliefs about their ability to control worry, rumination, and attention went from no control to strong control).
MCT patients also received around one fewer therapy session on average and recovered double as fast as the patients receiving CBT.
What do the results mean?
This is one of the largest studies on the difference between MCT and CBT. The results clearly show that MCT is more effective than CBT for depression and more cost-effective than CBT.
MCT could become the gold-standard treatment in the future because it is effective, fast, and prevents relapse into depression because of the change in metacognitive beliefs.
5) Comparing group MCT with group CBT for obsessive-compulsive disorder
“Group Cognitive-Behavior Therapy or Group Metacognitive Therapy for Obsessive-Compulsive Disorder? Benchmarking and Comparative Effectiveness in a Routine Clinical Service”
What is it about?
This study(11) examined group therapy treatment for obsessive-compulsive disorder, OCD. It also compared Metacognitive group therapy with Cognitive-behavioral group therapy.
Who participated?
125 OCD patients received group CBT, and 95 OCD patients received group MCT. Both group treatment courses lasted 12-weeks each.
What did they find?
The majority of patients who received CBT improved much from OCD symptoms, but 28% did not. A 28% not improved rate is already identified in CBT research: a significant proportion of OCD patients have minimal or no response to CBT (11).
The patients who received MCT improved significantly more than the CBT group, but 9,4 % did not.
22.3% more patients recovered with MCT compared to CBT.
MCT reduced non-responders to therapy by 10.5% compared with CBT. It means that 10.5 % fewer people did not recover from MCT compared to 28% who did not recover from CBT.
The results show that patients who received MCT group therapy improved much more over the 12-week course than the CBT groups. These results were not influenced by age, how many diagnoses the patients had, symptoms of depression, or medications they took.
The difference in response rates was statistically significant. For results to be statistically significant, it means you can feel confident that’s it real, and not that you just got lucky by chance.
What do the results mean?
The results mean that MCT is effective for treating OCD, and it can better help OCD patients who don’t respond to other therapies like CBT.
Note: People with OCD have a slightly different set of metacognitive beliefs, called fusion beliefs, which makes it harder for them to disqualify their intrusions (as is the case in CBT treatment for OCD). You can read more about Metacognitive therapy for OCD in this post.
Criticism of Metacognitive Therapy
Even though MCT has gained support from a growing body of research, critics argue that more rigorous studies are needed to determine its effectiveness and impact. Common concerns include:
Limited research
While there is evidence of MCT’s effectiveness, the overall research is still limited compared to other established therapies like Cognitive Behavioral Therapy (CBT).
Measurement accuracy
Assessing metacognitive beliefs and processes can be challenging as they are often abstract and difficult to measure.
Not enough long term results
Most studies have focused on short-term outcomes, and it is not yet well-established how effective MCT is in the long run
A “careless” approach
Traditional psychotherapy usually promote a different approach to thoughts and emotions than MCT. These therapies encourage reflection on thoughts with the goal of controlling unwanted thoughts.
MCT encourages a relaxed relationship with thoughts and feelings, which from a traditional approach’s perspective can seem as a careless and unproductive way of treating serious mental disorders.
If you want to read more about criticism of MCT and why it may not work, go to this post.
Book free intro session to learn how MCT can help you
Sources
- Schweiger JI, Kahl KG, Klein JP, Sipos V and Schweiger U (2019) Innovation in Psychotherapy, Challenges, and Opportunities: An Opinion Paper. Front. Psychol. 10:495. doi: 10.3389/fpsyg.2019.00495
- Wells, Metacognitive therapy for anxiety and depression, Guilford press, 2009
- Normann & Morina, The Efficacy of Metacognitive Therapy: A Systematic Review and Meta-Analysis, Front. Psychol., 14 November 2018 | https://doi.org/10.3389/fpsyg.2018.02211
- Nordahl, H., Borkovec, T., Hagen, R., Kennair, L., Hjemdal, O., Solem, S., . . . Wells, A. (2018). Metacognitive therapy versus cognitive–behavioural therapy in adults with generalised anxiety disorder. BJPsych Open, 4(5), 393-400. doi:10.1192/bjo.2018.54
- Wells, Metacognitive therapy for anxiety and depression, Guilford press, 2009
- Wells A (2019) Breaking the Cybernetic Code: Understanding and Treating the Human Metacognitive Control System to Enhance Mental Health. Front. Psychol. 10:2621. doi: 10.3389/fpsyg.2019.02621
- Normann & Morina, The Efficacy of Metacognitive Therapy: A Systematic Review and Meta-Analysis, Front. Psychol., 14 November 2018 | https://doi.org/10.3389/fpsyg.2018.02211
- Nordahl, H., Borkovec, T., Hagen, R., Kennair, L., Hjemdal, O., Solem, S., . . . Wells, A. (2018). Metacognitive therapy versus cognitive–behavioural therapy in adults with generalised anxiety disorder. BJPsych Open, 4(5), 393-400. doi:10.1192/bjo.2018.54
- Solem, S., Wells, A., Kennair, L. E. O., Hagen, R., Nordahl, H., & Hjemdal, O. (2021). Metacognitive therapy versus cognitive–behavioral therapy in adults with generalized anxiety disorder: A 9-year follow-up study. Brain and Behavior, 11, e2358. https://doi.org/10.1002/brb3.2358
- Callesen, P., Reeves, D., Heal, C. et al. Metacognitive Therapy versus Cognitive Behaviour Therapy in Adults with Major Depression: A Parallel Single-Blind Randomised Trial. Sci Rep 10, 7878 (2020). https://doi.org/10.1038/s41598-020-64577-1
- Papageorgiou C, Carlile K, Thorgaard S, Waring H, Haslam J, Horne L, Wells A. Group Cognitive-Behavior Therapy or Group Metacognitive Therapy for Obsessive-Compulsive Disorder? Benchmarking and Comparative Effectiveness in a Routine Clinical Service. Front Psychol. 2018 Dec 10;9:2551. doi: 10.3389/fpsyg.2018.02551. PMID: 30618972; PMCID: PMC6295517.


